
Just recently, the NFL did a sudden reexamination and update to its “Covid-19” testing protocols as far too many star players were testing positive and missing games. This obviously led to the games either having to be rescheduled or forfeited altogether which is a disaster for the ratings hungry league. According to the NFL, 94.6% of NFL players are vaccinated while nearly 100% of NFL personnel are vaccinated. Many of those players who have been testing positive are fully vaccinated. Two-thirds of the positive cases are asymptomatic while the rest have very mild symptoms. In fact, many players were frustrated as they felt they were perfectly capable of playing despite the positive label. However, a positive test result meant immediate quarantines and the loss of valuable players. With only four games left at the time and the games being critical for playoff standings, the NFL made some changes in order to avoid a PR and ratings nightmare:
As COVID forces NFL into lockdown, testing changes are being made to get infected players back quickly
“Another key change: Players with a technically positive test can also return to the facility depending on how low their viral load is — which is measured by a “cycle threshold” or “CT” value. If a player’s CT value is 35 or higher, they could register as COVID positive but not be considered infectious. With that in mind, the league and union agreed on a threshold that will allow players to return to the team with CT values of 35 or higher on tests.”
The NFL decided it needed to make its testing protocol easier for players to get back into the game sooner. Thus, they changed it so that any player with a Cycle Threshold (Ct) Value of 35 or higher could return to action as soon as possible. For those unfamiliar with the PCR Ct value, this is the number of cycles necessary in order for the fluorescent signal to cross the threshold above the background level. During this process, the starting material from the sample is doubled with every cycle. The higher the amount of cycles the PCR test is run at, the less accurate the results.
For a more in-depth look at Ct Values, please see this related post:
PCR Ct Values: Arbitrary & Meaningless

Somehow, even though the “SARS-COV-2” PCR tests are unable to determine infectiousness nor how sick one is, the NFL decided that any result with a Ct value of 35 or more meant that the player was not infectious and that they were ultimately well enough to play. The “SARS-COV2” PCR test, as authorized under the Emergency Use Act as they are not FDA-approved, can only be used qualitatively (a positive/negative result) but not quantitatively (how much “virus” is theoretically present). Knowing this, where would the NFL get the idea that PCR Ct values can say anything about the state of infectiousness in an individual or that this value can be used to measure so-called “viral” load?
It wasn’t from the CDC as they state very clearly that PCR tests are not to be used in this way:
Can a diagnostic RT-PCR test show how infectious one is?
“No. RT-PCR tests are used to identify and diagnose an active infection and cannot be used to show how infectious an individual person is.”
Can a Ct Value determine how much viral genetic material is present in an individual patient specimen?
“As of August 5, 2021, all diagnostic RT-PCR “tests that had received a US Food and Drug Administration (FDA) Emergency Use Authorization (EUA) for SARS-CoV-2 testing were qualitative tests. In a qualitative RT-PCR test, known amounts of virus are used during the development of the test to determine what Ct values are associated with positive and negative test results. A Ct value is generated when testing a patient specimen and is used to interpret a test as positive or negative but cannot be used to determine how much virus is present in an individual patient specimen.”
Can a Ct value predict how infectious an individual with Covid-19 is?
“No. Ct values should not be used to determine an individual’s viral load, how infectious an individual person may be, or when an individual person can be released from isolation or quarantine.
Although there is an association between Ct value and the amount of genetic material in a patient sample, attempting to correlate Ct values and the amount of virus in the original specimen is imperfect. Ct values can be affected by many factors other than viral load, including but not limited to improper collection or storage of the specimen, how the specimen was processed, or the sensitivity level of the test performed. Thus, a high Ct value can easily result from factors not related to the amount of virus in the specimen. Ct values should not be used to infer a relationship with the viral load from a person’s specimen, nor should they be used to determine the level of infection risk posed by a particular individual.”
https://www.cdc.gov/coronavirus/2019-ncov/lab/faqs.html
According to the CDC, the way the NFL is using and interpreting the PCR results is entirely inaccurate. Ct values can not be used for infectiousness, can not be used to determine “viral” load, and can not be used to determine when a person can be released from quarantine/lockdown.

How about the FDA? You will find a variation of this statement in all PCR EUA’s released:
“Positive results are indicative of the presence of SARS-CoV-2 RNA; clinical correlation with patient history and other diagnostic information is necessary to determine patient infection status. The agent detected may not be the definite cause of disease. Positive results do not rule out bacterial infection or co-infection with other viruses.”
It would seem that the FDA is very clear that the test results only indicate “SARS-COV-2” RNA was found and that this result does not tell how infectious one is or if the RNA detected is truly the cause of disease. The FDA, however, does allow manufacturers to set their own Ct values thus allowing the makers of the test to determine who is positive and who is not:
Who determines the Ct cutoff?
- The Ct cutoff is determined by the manufacturer of the test, not the state or laboratory performing the test. The cutoffs are reviewed during the submission process for the FDA’s Emergency Use Authorization (EUA). Once a test receives the EUA, the Ct cutoffs are set and cannot be changed by laboratories.
- Not all test manufacturers use the same Ct cutoffs, each test differs based on how it is designed and what part of the SARS-CoV-2 genetic material it targets for detection. Test manufacturers establish the cutoffs based on evaluation of their test with known positive and negative samples.
Why isn’t the Ct value reported on SARS-CoV-2 tests?
- The FDA EUA limits molecular diagnostic tests to report qualitative (positive/negative) of SARS-CoV-2 results and not quantitative (Ct value) results.
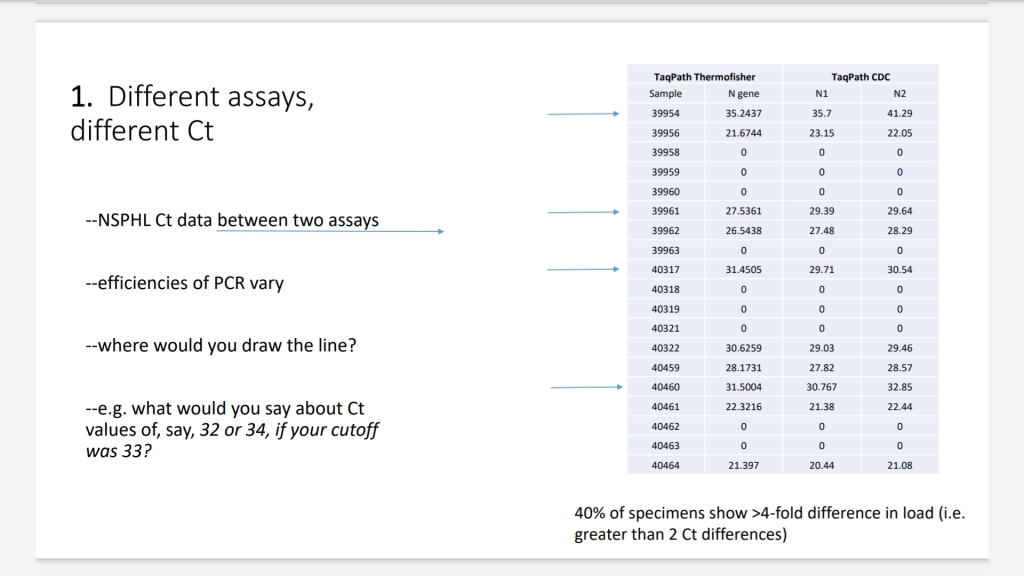
- Ct values and cutoffs differ by test and thus cannot be compared from one test to another. A specimen with a Ct=36 may be considered positive by one test but produce a different Ct value and be considered negative or indeterminate on another.
- Some RT-PCR tests do not use Ct values, but produce different values like relative light units (RLU) or cycle numbers (CN).
- No matter the method, all SARS-CoV-2 tests are reported qualitatively (positive/negative, etc).

In other words, while the FDA does not endorse the use of Ct values to determine infectiousness nor severity of illness, it does endorse the arbitrary determination of the Ct value cut-off by the manufacturers of each test to determine positivity. This means that results will vary between tests as they use different methods with differing Ct value cut-offs in order to label a person positive or negative. Thus, one could be positive for “SARS-COV-2” based on the Ct value for one test while entirely negative using a different test with the same Ct value.
In any case, if it wasn’t from the CDC nor the FDA, where did the NFL get this idea that Ct values can be used to determine infectiousness and a person’s “viral” load? It seems that this information may have come from the WHO. In January 2021, the WHO put out a notice for lab workers clarifying the interpretation of PCR test results. In it, they make a clear statement about “viral” load:
Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2
“WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.”
https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
From the (1) reference listed above regarding weak positive results:
Diagnostic testing for SARS-CoV-2
“Careful interpretation of weak positive NAAT results is needed, as some of the assays have shown to produce false signals at high Ct values. When test results turn out to be invalid or questionable, the patient should be resampled and retested. If additional samples from the patient are not available, RNA should be re-extracted from the original samples and retested by highly experienced staff. Results can be confirmed by an alternative NAAT test or via virus sequencing if the viral load is sufficiently high. Laboratories are urged to seek reference laboratory confirmation of any unexpected results.”
“Laboratories are encouraged to define their assays’ detection limits, and senior staff should recognize how disease prevalence alters the predictive value of their test results. Once the number of cases goes down, the positive predictive value will decrease, therefore the interpretation of tests should continue to be part of a stringent quality assurance scheme, with interpretation based on: timing of sampling, sample type, test specifics, clinical data and epidemiological data.”
https://www.who.int/publications/i/item/diagnostic-testing-for-sars-cov-2

It would appear that the WHO makes a distinction between Ct values and a supposed “viral” load. They claim high Ct values (inversely meaning low “viral” loads) can lead to false-positive results and that careful interpretation of the test results is needed. Unfortunately, the WHO does not state what Ct cut-off constitutes a high Ct value. However, we can infer this based on a final version document outlining the Target Product Profiles (TPP) for “Covid-19” diagnostics released by the WHO in September 2020. Let’s break down some key points:
Target product profiles for priority diagnostics to support response to the COVID-19 pandemic v.1.0
“Variable population characteristics are
expected, which will result in variable clinical sensitivity and specificity. Therefore, a limit of detection (LOD) that is based on anticipated viral loads in patient specimens and associated infectivity is critical to anticipate clinical utility. Reports in literature are variable: copies/reaction, copies/mL but most often cycle threshold (Ct) values. Correlation between viral load and transmissibility is not entirely clear – some reports cite inability to culture virus < 10^6. Therefore, we propose a POC test that can consistently detect the most infectious patients (e.g. LOD 10^6) in order to interrupt transmission. Test developers should use well characterized reference material and international standards, when available, to determine limits of detection.”
The WHO proposed a limit of detection of 10^6 for PCR testing, which is equal to a Ct value of 25 cycles. Just what is meant by the limit of detection? According to the Handbook for Immuniassay Technologies from 2018, the limit of detection (LOD) is defined as the “lowest concentration of an analyte in a sample that can be consistently detected with a stated probability (typically at 95% certainty).”
This means that the lowest acceptable level in order to detect “SARS-COV-2” reliably from any background noise would be a Ct of 25. In the same document, the WHO makes the distinction that a Ct value anywhere from 25-30 would be acceptable while a desirable level is anything equal to or greater than a Ct value of 30.

Why does this matter? The higher the Ct value, the more background noise interference is generated and the less reliable the results. Most “Covid-19” tests are run at a Ct value of 40 cycles, with some going as high as 50. Obviously, the WHO would love the tests to reliably detect “SARS-COV-2” at much higher Ct levels in order to justify running PCR tests through that many cycles. However, this is not the case and many have called for the tests to be run at 30 cycles or lower. Even Fauci himself stated any PCR result over 35 Ct was nothing but “dead nucleotides.” Perhaps knowing that these PCR results are more inaccurate the higher the amount of cycles used allowed the NFL the confidence to claim any player with a Ct value of 35 or more is allowed to play?
It is interesting to note in this document that the WHO states that cross-reactions with “SARS-COV-1,” a “virus” that only shares a 79% relationship with “SARS-COV-2,” is considered acceptable.

This means that any result that would have been detected as “SARS-COV-1” in the past is now considered to be “SARS-COV-2.” Why would the WHO make this distinction?


The WHO allows for cross-reactivity to “SARS-COV-1” as they claim (or rather ASSUME) it is no longer circulating. However, if they did not routinely test for “SARS-COV-1” leading up to this “pandemic” and now consider any cross-reactivity to be “SARS-COV-2,” how would they know whether or not the old strain is currently circulating? Why is any level of cross-reactivity to other “viruses” in any way acceptable? Could it be due to the fact that the “SARS-COV-1” genome was used as a reference to build the “SARS-COV-2” genome? This should immediately tell you that these tests are not specific and therefore not as accurate as they are claimed to be.
Also of note from this WHO document is the sample storage conditions. The WHO allows for one or more preservatives/”viral” transport medium to be used with each sample.

If you know anything about “viral” transport medium, you will understand it is a collection of added chemicals and RNA from various outside sources. This is how one manufacturer of VTM for “SARS-COV-2” explains it:
“Our Viral Transport Medium is based on Hanks Balanced Salt Solution (HBSS) with Calcium and Magnesium and contains heat-inactivated Fetal Bovine Serum, Gentamycin and Amphotericin B. The composition and the manufacturing of the Viral Transport Medium follow the WHO and the CDC recommendations.”
https://www.clinisciences.com/en/read/newsletter-26/covid-19-viral-transport-medium-2267.html

If the sample being used for PCR amplification is already contaminated with substances such as baby cow blood (which contains its own RNA) along with who knows what else in the undefined medium(s), how can the results ever be viewed as accurate? It is well known that fetal bovine serum (FBS) alone is highly variable in content. Perhaps just the addition of this one substance allows for the varying results between tests and labs or even the same lab using the same sample and test?
Whatever the case may be, the WHO is clearly stating things about the interpretation of PCR results that are not supported by the evidence nor the intended use of the product. This is obviously a problem when one of the main organizations making decisions during this “pandemic” is releasing unreliable and false information. Fortunately, the American Association of Clinical Chemistry recently released a statement as to why the WHO’s proposals are problematic and why Ct values are not to be used for patient management:
How to Say No to Reporting Ct Values
AACC has advocated against using Ct values for managing COVID-19 patients, and new evidence supports a cautious approach.
“As the world grapples with the ongoing COVID-19 pandemic, public health organizations are trying to help clinicians grasp how best to treat their patients with the most accurate and useful testing possible. One proposed recommendation, as set out by the World Health Organization, is to use cycle threshold (Ct) values set by quantitative polymerase chain reaction (qPCR) as a performance target for newly developed diagnostic technologies.
In this way, the WHO uses Ct values as a surrogate for the level of viral load. WHO has proposed a Ct value of 25 as the minimum level of virus that should be detected by a point-of-care diagnostic test. Ct also has been proposed by some to be used to tell who has a high viral load and might be at higher risk for severe disease, who might be infectious and likely to spread disease, and who can be released from quarantines.
AACC has come out against using Ct values for managing patients with COVID-19. In a statement published in July 2021, AACC emphasized that SARS-CoV-2 tests are not standardized in any one country, let alone around the world (www.aacc.org/science-and-research/covid-19-resources). The same Ct value can therefore mean widely different things for different tests, potentially leading to inappropriate patient care.
“I can understand why people would want to compare Ct values, but there is a potential for harm when looking at an assay that is not validated to be quantitative. SARS-CoV-2 tests are validated to be qualitative,” said Deborah Payne, PhD, MT(ASCP), ABMM, DABCC, FAACC, a clinical consultant and a member of the AACC group that wrote the AACC Ct values statement.
NO TWO NOSTRILS ARE ALIKE
Payne said that it’s natural to think Ct values can be used to determine severity of COVID-19. That’s because Ct values are routinely used to detect viral burden in infections like HIV and hepatitis C and B viruses. That number is valuable because collection of urine or blood is uniform, she said. However, “collection from a swab is not.”
To start, not every swab, nose, or even each nostril in the same person is the same. “There’s biological variance between the nasal cavities. You can have one nostril with detectable SARS-CoV-2 and the other nostril without, which is why the recommendation is to swab both sides of the nose,” she said.
Clinical laboratory professionals also don’t yet have the data to understand the optimal conditions for taking samples for a PCR test for a respiratory disease. Some urine assays are best taken in the morning, for example, and some blood samples drawn after a patient fasts. “We don’t really know enough about the respiratory system when it comes to this kind of testing and what the optimal time of day is to collect a sample,” Payne said. “We don’t know enough about respiratory virus shedding to know whether there’s a particular time it’s better to take a test, or whether there’s a difference between morning and evening, and how that will affect results.”
On top of not being able to adjust for differences in swabs and nostrils, and not having established optimal sampling conditions, the sheer number of assays given emergency use authorization (EUA) in the U.S. and the equivalent in other countries means that there are no standards across testing platforms and laboratories either. They aren’t calibrated against each other, so a Ct value of 25 on one test could mean high viral load in a patient in California, low viral load in a patient in New Jersey, and somewhere in between in a patient in Australia.
Without calibration, a Ct value is “virtually meaningless,” said Jim Francis Huggett, PhD, of the U.K. National Measurement Laboratory at LGC, and professor in analytical microbiology at the University of Surrey, who set out to find out just how meaningless it is.
UNCALIBRATED TESTS LEAD TO WILDLY DIFFERENT RESULTS
Huggett revealed the trouble with relying on Ct values by leading a team of researchers to study the differences in SARS-CoV-2 tests from labs around the world. One aim was to determine how WHO’s suggested Ct cutoff of 25 impacts coronavirus test performance, if at all.
In the resulting paper, which was published in AACC’s journal Clinical Chemistry, researchers analyzed the results of more than 6,000 patients who underwent PCR testing at clinical laboratories in the U.K., Belgium, and the Republic of Korea (Clin Chem 2021; doi: 10.1093/clinchem/hvab21). For this particular study, all PCR tests used were considered to have 100%
clinical sensitivity.
When Huggett’s team interpreted the test results using WHO’s cutoff, the tests’ sensitivity dropped, varying from approximately 16% to 90%, depending on the patient cohort. “There were three different groups at three different labs and we got three distinct differences,” Huggett said.
The researchers also conducted analysis of data from 732 additional laboratories and found that an individual Ct value can correspond to widely different viral loads depending on the lab. For example, a Ct value range of 25 to 30 should correspond to 106 copies of SARS-CoV-2/mL. But researchers also found that the Ct range can correspond to as many as 108 copies to as few as 103 copies.
“That’s a range of a hundred thousand fold difference,” he said. “It’s chaos.”
WHAT TO DO WITH CT VALUES
AACC isn’t the only organization that has come out against the WHO Ct value recommendation. In a December letter to the editor in Clinical Infectious Diseases, the American College of Pathologists also cautioned against using Ct values for COVID-19, citing many of the same concerns as AACC, including variables in testing collection, no quantitative assay standardization, the wide range of Ct values among laboratories, and that some PCR tests use isothermal amplification methods and therefore don’t produce Ct values at all.
This doesn’t mean that Ct values have no use when it comes to COVID-19. “As long as you control the experiments, you can use a Ct value in your lab as a guide to compare one result to another,” Huggett said. “But as soon as you try to compare a number between laboratories, it means nothing because of the large amounts of variation,” he added. “If you’re going to use the Ct value, you need to work out what is your own scale, and be aware of how it may differ over time and cognizant of the limitations of using such an approach.”
Right now, epidemiologists can also use Ct values of COVID tests if they’re “looking at a large number of points. Then if there’s an outlier, that outlier can be accounted for,” said Payne. It can give a bigger picture of the virus in one population without having an impact on individual patient care.
For example, researchers used mathematical modeling to show that capturing the Ct values of positive SARS-CoV-2 PCR results could give a real-time estimate of the growth rate of the virus in a community (Science 2021; doi: 10.1126/science.abh0635). “The Ct value is a measurement with magnitude, which provides information on underlying viral dynamics,” the authors wrote. “Although there are challenges to relying on single Ct values for individual-level decision-making, the aggregation of many such measurements from a population contains substantial information. These results demonstrate how one or a small number of random virologic surveys can be best used for epidemic monitoring.”
For Ct values to be useful for managing patients on a worldwide scale, though, there needs to be a standard calibration and sample standardization, much like what happened in order for laboratories to use Ct scores for HIV and other diseases.
TALKING TO CLINICIANS ABOUT CT VALUES IN COVID-19
The AACC statement does acknowledge that laboratories are “in a difficult position,” and that “there may also be pressure from their clinical colleagues to report or, at a minimum, have access to Ct values.” For laboratories that decide to report Ct values, AACC suggests including an interpretative comment with the test results:
The utilization of Ct values to guide patient management is discouraged. Correlation with viral load, viral burden, or infectivity has not been established for qualitative SARS-CoV-2 tests. Numerous factors such as biological variance, adequacy of sample, time of exposure, instrumentation, methodology, lack of certified reference material, and regulatory factors influence the Ct values detected in qualitative SARS-CoV-2 assays. Therefore, AACC discourages reporting or disclosing Ct values to guide patient management.
Meanwhile, as WHO considers making a specific Ct value minimum recommendation, the U.S. Centers for Disease Control and Prevention has not. In their COVID-19 FAQ for laboratories, updated on August 25, 2021, they stated that “Ct values should not be used to determine an individual’s viral load, how infectious an individual person may be, or when an individual person can be released from isolation or quarantine.”
Despite such a blunt statement, a contrarian view by WHO could still hold sway, especially in countries without their own robust public health organizations, Huggett said. Established use of Ct values in other conditions also can muddy the waters. Huggett knows it can be difficult to explain to clinicians why the logical conclusion that the Ct might be used to guide management of COVID-19 patients is wrong—he himself is married to a medic, he joked. He also doesn’t want to knock Ct values completely as they do have some value now.
“To say it’s rubbish is incorrect. If it’s one laboratory and standardized, that could be fit for purpose,” he said. “What’s not fit for purpose is using the same number in different labs. It has to be very specific to that laboratory.”
https://www.aacc.org/cln/articles/2021/december/how-to-say-no-to-reporting-ct-values

The position by the AACC is very clear: Ct values should not be used to infer infectivity, “viral” load, nor severity of disease. These values, as far as clinical care is concerned, are utterly meaningless. As stated in the article, the College of American Pathologists (CAP) also came to the same conclusion in December 2020:
What are the downsides of reporting Ct-values?
“Ct-values are not standardized across specimen sources, testing platforms, or laboratories. Although Ct-values have been correlated with prognosis and infectivity in some studies, there is an opportunity to over-interpret results or attribute false precision to a Ct-value. Other studies have identified infectious virions can be present in specimens that yield high Ct-values.”
Should Ct-values be reported for SARS-CoV-2 PCR testing?
“There is not currently formal guidance as to whether the Ct-value result of a PCR test used to detect SARS-CoV-2 should or should not be reported along with the interpretation of the result. All FDA EUA IVDs for the detection of SARS-CoV-2 are currently authorized for only qualitative interpretation. Generally, lower Ct-values are associated with higher viral burden in a sample, but inferring clinically meaningful information based on a Ct-value can be challenging.”
Even the IDSA and the AMP offered similar insights as I detailed here:
The IDSA and AMP Joint Statement Destroying PCR Tests
In Summary:
- The NFL recently changed its “Covid-19” testing protocols in order to make it easier for positive players to continue playing
- Players with a technically positive test can return to the facility depending on how low their “viral” load is — which is measured by a “cycle threshold” or “CT” value
- If a player’s CT value is 35 or higher, they could register as “COVID” positive but not be considered infectious
- With that in mind, the league and union agreed on a threshold that allowed players to return to the team with CT values of 35 or higher on tests
- According to the CDC, PCR cannot be used to show how infectious an individual person is
- The tests are qualitative, not quantitative, and cannot be used to determine how much “virus” is present in an individual patient specimen
- The CDC also states Ct values should not be used to determine:
- an individual’s “viral” load
- how infectious an individual person may be
- or when an individual person can be released from isolation or quarantine
- Attempting to correlate Ct values and the amount of “virus” in the original specimen is imperfect
- A high Ct value can easily result from factors not related to the amount of “virus” in the specimen
- Ct values should not be used to infer a relationship with the “viral” load from a person’s specimen, nor should they be used to determine the level of infection risk posed by a particular individual
- According to the FDA disclaimers on PCR tests:
- Positive results are indicative of the presence of “SARS-CoV-2” RNA
- Clinical correlation with patient history and other diagnostic information is necessary to determine patient infection status
- The agent detected may not be the definite cause of disease
- Positive results do not rule out bacterial infection or co-infection with other “viruses”
- The Ct cutoff is determined by the manufacturer of the test
- Not all test manufacturers use the same Ct cutoffs, each test differs based on how it is designed and what part of the “SARS-CoV-2” genetic material it targets for detection
- The FDA EUA limits molecular diagnostic tests to report qualitative (positive/negative) of SARS-CoV-2 results and not quantitative (Ct value) results
- Ct values and cutoffs differ by test and thus cannot be compared from one test to another
- According to the WHO, the cycle threshold (Ct) needed to detect “virus” is inversely proportional to the patient’s “viral” load
- Results can be confirmed by an alternative NAAT test or via “virus” sequencing if the “viral” load is sufficiently high
- Careful interpretation of weak positive NAAT results is needed, as some of the assays have shown to produce false signals at high Ct values
- Laboratories are encouraged to define their assays’ detection limits, and senior staff should recognize how disease prevalence alters the predictive value of their test results
- Once the number of cases goes down, the positive predictive value will decrease
- Variable population characteristics are expected, which will result in variable clinical sensitivity and specificity
- Therefore, a limit of detection (LOD) that is based on anticipated “viral” loads in patient specimens and associated infectivity is critical to anticipate clinical utility
- Reports in literature are variable: copies/reaction, copies/mL but most often cycle threshold (Ct) values
- Correlation between “viral” load and transmissibility is not entirely clear – some reports cite inability to culture virus < 10^6.
- Therefore, the WHO proposes a POC test that can consistently detect the most infectious patients (e.g. LOD 10^6) in order to interrupt transmission
- According to the AACC, the World Health Organization has proposed to use cycle threshold (Ct) values set by quantitative polymerase chain reaction (qPCR) as a performance target for newly developed diagnostic technologies
- In this way, the WHO uses Ct values as a surrogate (i.e substitute; stand-in) for the level of “viral” load
- WHO has proposed a Ct value of 25 as the minimum level of “virus” that should be detected by a point-of-care diagnostic test (what the proposed maximum Ct value is, they don’t say…)
- In a statement published in July 2021, AACC emphasized that “SARS-CoV-2” tests are not standardized (cause something to conform to a standard; determine the properties of by comparison with a “gold” standard) in any one country, let alone around the world
- The same Ct value can therefore mean widely different things for different tests, potentially leading to inappropriate patient care
- According to Deborah Payne, PhD, MT(ASCP), ABMM, DABCC, FAACC, a clinical consultant and a member of the AACC group that wrote the AACC Ct values statement, there is a potential for harm when looking at an assay that is not validated to be quantitative and “SARS-CoV-2” tests are only “validated” to be qualitative (i.e. positive or negative result only)
- Collection from a swab is not uniform in the material aquired
- Payne states that there’s biological variance between the nasal cavities where you can have one nostril with detectable “SARS-CoV-2” and the other nostril without, which is why the recommendation is to swab both sides of the nose
- Clinical laboratory professionals also don’t yet have the data to understand the optimal conditions for taking samples for a PCR test for a respiratory disease
- Payne also states that they don’t know enough about respiratory “virus” shedding to know whether there’s a particular time it’s better to take a test, or whether there’s a difference between morning and evening, and how that will affect results
- On top of not being able to adjust for differences in swabs and nostrils, and not having established optimal sampling conditions, the sheer number of assays given emergency use authorization (EUA) in the U.S. and the equivalent in other countries means that there are no standards across testing platforms and laboratories either
- The tests are not calibrated against each other, so a Ct value of 25 on one test could mean high “viral” load in a patient in California, low “viral” load in a patient in New Jersey, and somewhere in between in a patient in Australia
- According to Jim Francis Huggett, PhD, of the U.K. National Measurement Laboratory at LGC, and professor in analytical microbiology at the University of Surrey, without calibration, a Ct value is “virtually meaningless,”
- Huggett lead a team of researchers to analyze the results of more than 6,000 patients who underwent PCR testing at clinical laboratories in the U.K., Belgium, and the Republic of Korea
- For this particular study, all PCR tests used were considered to have 100% clinical sensitivity
- When Huggett’s team interpreted the test results using WHO’s cutoff of 25, the tests’ sensitivity dropped, varying from approximately 16% to 90%, depending on the patient cohort
- “There were three different groups at three different labs and we got three distinct differences,” Huggett said
- The researchers also conducted analysis of data from 732 additional laboratories and found that an individual Ct value can correspond to widely different “viral” loads depending on the lab
- In a December letter to the editor in Clinical Infectious Diseases, the American College of Pathologists also cautioned against using Ct values for “COVID-19,” citing many of the same concerns as AACC, including:
- Variables in testing collection
- No quantitative assay standardization
- The wide range of Ct values among laboratories
- Some PCR tests use isothermal amplification methods and therefore don’t produce Ct values at all
- Huggert stated that as soon as you try to compare a number between laboratories, it means nothing because of the large amounts of variation and that if you’re going to use the Ct value, you need to work out what is your own scale, and be aware of how it may differ over time and cognizant of the limitations of using such an approach
- Researchers have used mathematical modeling to show that capturing the Ct values of positive “SARS-CoV-2” PCR results could give a real-time estimate of the growth rate of the “virus” in a community
- For Ct values to be useful for managing patients on a worldwide scale, though, there needs to be a standard calibration and sample standardization, much like what happened in order for laboratories to use Ct scores for HIV and other diseases (which is a whopper of a lie as HIV tests are not standardized)
- The AACC recommended adding this disclaimer to any Ct Value:
- The utilization of Ct values to guide patient management is discouraged. Correlation with viral load, viral burden, or infectivity has not been established for qualitative SARS-CoV-2 tests. Numerous factors such as biological variance, adequacy of sample, time of exposure, instrumentation, methodology, lack of certified reference material, and regulatory factors influence the Ct values detected in qualitative SARS-CoV-2 assays. Therefore, AACC discourages reporting or disclosing Ct values to guide patient management
- The CDC also stated that Ct values should not be used to determine an individual’s “viral” load, how infectious an individual person may be, or when an individual person can be released from isolation or quarantine
- Huggert concluded that Ct values are not fit for the purpose of using the same number in different labs as it has to be very specific to that laboratory
- According to the College of American Pathologists (CAP), Ct-values are not standardized across specimen sources, testing platforms, or laboratories
- Other studies have identified “infectious virions” can be present in specimens that yield high Ct-values
- All FDA EUA IVDs for the detection of “SARS-CoV-2” are currently authorized for only qualitative interpretation
- Generally, lower Ct-values are associated with higher “viral” burden in a sample, but inferring clinically meaningful information based on a Ct-value can be challenging
- Both the Infectious Disease Society of America (IDSA) and the Association for Molecular Pathology (AMP) have come out against the use of Ct values citing similar reasoning

If we are keeping count, the CDC, AACC, CAP, IDSA, and the AMP all state that PCR Ct values can not and should not be used to determine infectivity, “viral” load, and disease severity. The FDA has only allowed these tests out on the basis of the Emergency Use Authorization for qualitative (positive/negative) but not quantitative (how much “virus” is present) purposes. They state on the tests that the detection of “SARS-COV-2” RNA does not mean it is the cause of a person’s symptoms. Obviously, the NFL and the WHO are playing fast and loose with the rules which is par for the course for both organizations. There are many reasons for the statements against the use of Ct values such as the lack of standardization among tests and labs, the arbitrary determination of the limit of detection and Ct cut-off by the manufacturers of the tests themselves, the variability in the sampling conditions, and the many factors outside of “viruses” that can affect the Ct value results. However, the biggest reason against the use of PCR tests and Ct values is that no test has ever been validated and calibrated against purified/isolated “SARS-COV-2.” The “virus” that the tests are supposedly detecting has never been scientifically proven to exist. Thus, if one takes all of this information into account, it should be relatively easy not just to say no to the use of Ct values as the AACC suggests, but to also say no to the PCR test itself as well.

“qualitativrly” – you can delete this message. Just letting you know about a typo while I read
LikeLiked by 1 person
Thanks for letting me know! I hate typos. My proofreading skills are slipping. 😦
LikeLiked by 1 person
I can’t say anything. If I don’t listen to (using text-to-speech apps) and read it thru, typos & bad grammar become way too obvious.
LikeLiked by 1 person
I’m talking about going thru my own articles. Wasn’t clear enough. Sorry.
LikeLiked by 1 person
No worries, I understood. 🙂
LikeLike
I’ve finished reading now. I shake my head reading through all your quotes. I’m sure you know they literally tell you what the inventor of PCR said, that it cannot tell you if you’re infectious or if what it found causes any illness. That’s what he said! That’s what they’re saying! But they’re still using the blasted thing!!! So frustrating! Just seeing how meaningless the cycle threshold is and the fact there is no standardisation amongst companies only further highlights the farce this all is. And it continues nonetheless. Damn irritating!
LikeLiked by 1 person
It is extremely frustrating. There is this doublespeak going on where they say Ct can’t be used for various reasons while they still use it to determine one positive. They want to have their cake and eat it too, so to speak. It’s ridiculous.
LikeLike
Great article, by the way
LikeLiked by 1 person
Thanks, I appreciate it! I had a difficult time with this one for some reason. I tried to keep the message and through line consistent as best I could. I may not have been entirely successful as I keep seeing things I can change or improve but at some point you have to let it go and just get the information get out there. I can always revise things later if necessary. The info is too important to sit on. Thanks for all the input! 🙂
LikeLike
Yes indeed. The perfect “test” to manipulate for the outcome you want.
LikeLiked by 1 person
I felt like putting test in quotations throughout the article but I got lazy. 😉
LikeLike
You did a-good outline Misto. I am going to have more to say – This article shows what a fraud this is and the logical fallacies involved. Amazing how the NFL playoffs are upon us and suddenly the concern is making sure each team has all of its players available. If there was a real pandemic would changing the protocols be the concern. 2/3 of personnel tested are asymptomatic – right there they are telling you there is no virus causing sickness. Then they go on to say vaccinated are testing positive. Someone is making lots of money who create all of these products and who knows how much damage these products are causing
LikeLiked by 1 person
Absolutely. What is happening in the NFL goes a long way towards exposing this scam for what it is. Many aspects contradict the official narrative. Even the chief medical officer for the NFL destroyed the asymptomatic lie by claiming it does not exist in the NFL. The official narrative is falling apart.
LikeLike
From the article According to the CDC how the NFL is testing and interpreting results is entirely inaccurate. Which extrapolated out is how every lab, testing center, medical office on this planet is performing the tests
LikeLiked by 1 person
There was also mentioned by the AACC. lack of CERTIFIED REFERENCE MATERIAL. You know what word is always missing. Causation. Its just test test test. And no one ever says a positive result is causation for xyz
LikeLiked by 1 person
Exactly. They cannot claim causation based on the results which is why the FDA had to put the disclaimer that a positive result does not mean what was detected is actually causing disease. In other words, the results are absolutely meaningless. Sadly, people still line up to have their brains poked with giant Q-tips.
LikeLike
Just to ask, you have great articles on the PCR trash. Did you do any on the antigen “tests” or the lateral flow “tests”?
LikeLiked by 1 person
I haven’t really delved into them much. I’ve focused more on PCR and antibody tests. Like the antibody tests, the antigen/lateral flow tests are admitted not to be as accurate as PCR, and we know how inaccurate PCR is…so they must be pretty bad. 😉
LikeLiked by 1 person
Dude, I got no one else to talk to about this. Forgive me for what I say next if it’s nonsense. So the mythical entity, SARS-Cov-2, has never been found in entirety in reality, never been purified and shown to cause anything. I’ve found no original papers on the development of this particular lateral flow test or antigen test. They claim to it uses conjugated labels (no idea!) and antibodies to bind to viral antigens. They say the antigen the lateral flow tests react to is the proteins in covid. I don’t know if this means the proteins they think surround the viral dna/rna, or the protein that should produced when the viral dna/rna hijacks the cell’s machinery (their wording). According to the central dogma of genetics, dna makes rna which makes proteins. So a virus should make proteins, right? But they claim viruses, the viral dna/rna just makes itself???
My issue (one of my many issues) is that they never found sars-cov-2 and found broken bits of genetic mess. They didn’t find and purify an individual virus, a length of rna surrounded by protein. And they don’t make the whole thing in anything but a computer programme. So if the lateral flow test looks for target protein, what protein could it possibly be looking for??? what are the chemicals in the antigen “tests” reacting to?
The story is the PCR “tests” look for fragments of genetic code. Lateral flow tests or antigen tests doesn’t look for genes, so it can’t be looking for the rna of the mythical beast, Sars-Cov-2. So it’s looking for what protein?
The antigen “test” itself, at least what it’s looking for. It’s supposed to look for KNOWN antigens. That rules out a novel coronavirus, right? I just can’t understand what’s going on.
You may not either. But I’ve got nowhere else to vent my confusion that even has a chance of getting an intelligent response, if any. Am I making sense? Is my reasoning flawed?
LikeLiked by 1 person
The antigens/proteins said to belong to “SARS-COV-2” are just as mythical and theoretical as the “virus” itself and antibodies. None of these have been proven to exist in reality. They just look at chemical reactions and infer meaning from them. This is why these results are so inaccurate. They are not specific to anything at all.
LikeLiked by 1 person
Damn. Here I am overthinking this rubbish, and you just say “hey dude, just smell the crap. It stinks.” Simply said. It’s all fiction. Thanks man.
LikeLiked by 1 person
Lol, that’s a good way of putting it. Everything is theoretical BS. They can not observe “viruses,” antigens, antibodies, etc. They assume these things exist and that the chemical reactions which occur in a laboratory are proof these unseen particles are present. They then create stories around the results.
LikeLiked by 1 person
I did do a Facebook post in the past it seems:
LikeLiked by 1 person
Damn, not on facebook.
LikeLiked by 1 person
I can’t blame you for not being on FB. Here is a copy/paste of the post:
“From the BMJ:
“MASS TESTING OF PEOPLE WITHOUT COVID-19 SYMPTOMS IS “NOT AN ACCURATE WAY OF SCREENING THE GENERAL POPULATION,” a senior figure at the Department of Health and Social Care has said in a letter seen by The BMJ (see Related content).
THE COMMENTS WERE MADE BY JAMES BETHELL, ONE OF ENGLAND’S HEALTH MINISTERS, in response to a letter from an MP raising concerns ABOUT BLANKET POLYMERASE CHAIN REACTION (PCR) TESTING on behalf of a constituent.
In his letter Bethell stated that “SWAB TESTING PEOPLE WITH NO SYMPTOMS IS NOT AN ACCURATE WAY OF SCREENING THE GENERAL POPULATION, AS THERE IS A REAL RISK OF GIVING FALSE REASSURANCE.” He added, “WIDESPREAD ASYMPTOMATIC TESTING COULD UNDERMINE THE VALUE OF TESTING, AS THERE IS A RISK OF GIVING MISLEADING RESULTS. Rather, only people WITH COVID-19 SYMPTOMS should get tested.”
“However, experts have argued that it does not make sense that lateral flow tests—WHICH ARE FAR LESS ACCURATE THAN PCR TESTS—ARE CONSIDERED GOOD ENOUGH FOR MASS ASYMPTOMATIC TESTING, WHILE PCR TESTING IS BEING AVOIDED BECAUSE OF ITS POTENTIAL FOR FALSE REASSURANCE.
Jon Deeks, professor of biostatistics at the University of Birmingham and leader of the Cochrane Collaboration’s covid-19 test evaluation activities, said, “There are particular concerns about false reassurance. IT DOESN’T MAKE SENSE THAT THE GOVERNMENT IS CONCERNED ABOUT FALSE REASSURANCE FOR PCR TESTS BUT NOT LATERAL FLOW TESTS.
“LATERAL FLOW TESTS ARE GOING TO GIVE MORE FALSE REASSURANCE THAN PCR TESTING, BECAUSE THEY ARE LESS ACCURATE. It’s good to see the government is concerned about false reassurance, but haven’t they got this the wrong way around?”
“THE LAST THING anybody should be encouraged to entertain after an Innova test result, WHETHER POSITIVE OR NEGATIVE, IS CERTAINTY, LET ALONE ‘MORE’ OF IT.”
https://www.bmj.com/content/371/bmj.m4916
Related BMJ article:
“The rapid test kits most widely used in UK universities, schools, and care homes DETECT JUST 48.89% OF COVID-19 INFECTIONS IN ASYMPTOMATIC PEOPLE when compared with a polymerase chain reaction (PCR) test, real world data from the Liverpool pilot have shown.
The Innova Lateral Flow SARS-CoV-2 antigen test FAILED TO DETECT THREE IN 10 CASES WITH THE HIGHEST VIRAL LOADS, in preliminary data released from the field evaluation of testing in asymptomatic people.1”
“Jon Deeks, professor of biostatistics at the University of Birmingham and leader of the Cochrane Collaboration’s covid-19 test evaluation activities, told The BMJ, “These are the first results for this test in asymptomatic people. NORMALLY, WE WOULD ASCERTAIN HOW WELL A TEST WORKS BEFORE ROLLING IT OUT IN A NATIONWIDE PROGRAMME. THESE FINDINGS RAISE CONCERNS THAT BOTH THE GOVERNMENT’S AND INDIVIDUALS’ EXPECTATIONS ABOUT HOW WELL THIS TEST WORKS ARE NOT GOING TO BE MET.”
“THE LATERAL FLOW TESTS MISSED A THIRD OF PEOPLE WITH HIGH VIRAL LOAD who had Ct scores (cycle threshold, a measure of virus) below 25—but seven of 15 cases with Ct scores of 20-25 were missed, giving a sensitivity of only 47% in this group (21% to 73%). In people with Ct scores of 25-30, six of seven cases were missed—a sensitivity of 14% (0.4% to 58%). Deeks remarked, “WE ARE SEEING THAT IT IS REALLY VERY POOR AT DETECTING COVID IN ASYMPTOMATIC CASES, EVEN THOSE WITH A HIGHER VIRAL LOAD.”
https://www.bmj.com/content/371/bmj.m4848?ijkey=2d10010f247b79bcfac7b20f18837671ba1ec0ec&keytype2=tf_ipsecsha
Finally, also from the BMJ:
“Criticism of the Liverpool lateral flow testing pilot has focused on “false negatives”, BUT “FALSE POSITIVES” ARE ALSO A PROBLEM. From the available data, ONE IN TWO OF THE POSITIVE RESULTS BY LFT IN LIVERPOOL WILL BE “FALSE POSITIVES”. People with a positive test result are instructed to self-isolate and TO GET A CONFIRMATORY PCR”
“The FAQs simply state “THERE IS A POSSIBILITY THAT SOME PEOPLE WHO TEST POSITIVE WITH LFT ARE ‘FALSE POSITIVE’ AND THE GOLD STANDARD PCR TEST WILL IDENTIFY THESE.” Annex B says “The virus prevalence is around 1% in the country, SO WE EXPECT AROUND 7 TRUE POSITIVES AND 4 FALSE POSITIVES FOR EVERY 1000 PEOPLE TESTED.”
https://www.bmj.com/content/371/bmj.m4744/rr
As you can clearly see, they are using one inaccurate test (Lateral Flow) to cover up the faults in another inaccurate test (PCR) when doing mass testing.
You’re worried that the PCR test can not do accurate mass testing? Don’t worry about it. The lateral flow rapid test will be used to pick up any missed cases much more rapidly.
You’re concerned about the accuracy of the Lateral Flow tests in regards to mass testing? Don’t worry about it. The more “accurate” PCR test is there to pick up any missed cases more effectively.
Do you see this circular nonsense?
They are using one inaccurate test to back up another inaccurate test, which is then used to back up the first inaccurate test.
This is exactly why we have a TESTING PANDEMIC and not a “viral” one.”
LikeLiked by 1 person
You been at this game of using their own words against for some time, huh? Of course I’m keeping it! GRIN! I know, that was the plan! Thanx.
LikeLiked by 1 person
Yes, quite some time. I just started this blog 4 months ago but I’ve been researching for years. I decided to start doing posts on FB once this “pandemic” started to share with others what I have learned. Then FB censorship hit and forced me to create this blog. I’ve been redoing and updating old posts while also adding new ones in here and there. It has been a great refresher for me and a rewarding experience. 🙂
LikeLiked by 1 person
Well, I’m blessed by your work. Thank you. Let me know if you know of any alternatives to wordpress that will allow videos from sites other youtube & bitchute to be embedded in the article, please. Can’t seem to do it in WP.
Again, thanks for sharing your work.
LikeLiked by 1 person
Thanks for the support! I will let you know if I come across anything 🙂
LikeLiked by 1 person