
Most of the infections linked to human cancers are common in human populations; they are ubiquitous. They were present during the whole human evolution process.”
Harald Zur Hausen
For many decades, scientists had been trying to pin cancer on “viruses.” They attempted to link both herpes simplex and HIV to cancer but they just could not find convincing enough “proof” to make those hypotheses stick. In 1968, the National Cancer Institute (NCI) created a Special Virus Cancer Program which attempted to identify human cancer “viruses” so that it would be possible to vaccinate against and prevent these conditions. However, that project ended in failure and by 1980, the scientific community had come to an agreement that the efforts to pin cancer on “viruses” were fruitless:
“Despite more than a decade of research, however, the effort largely failed, and by the late 1970s, many researchers had soured on the idea. When the program was terminated in 1980, a medical consensus had emerged that viruses were not a significant cause of human cancers.”
https://www.cancerresearch.org/en-us/blog/august-2014/when-aids-was-a-cancer
Fortunately for those who held on to promoting this fraudulent connection between “viruses” and cancer, German virologist Harald Zur Hausen came along in 1983 to save the day. This man was credited with discovering the so-called link between the human papillomavirus (HPV) and cervical cancer. He did so with his “discovery” of hybridized cloned DNA fragments said to be HPV in some cervical cancer patients. However, even with Zur Hausen’s apparent discovery of this supposed link, many were very skeptical of his results, and for good reason.
A brief bit of background on his work first:
“Zur Hausen began his quest by looking for viruses in human genital warts, leading to the discovery of a new type of papillomavirus, which he called HPV-6 (versions one to five had already been discovered). Much to his disappointment, his team couldn’t find HPV-6 in any cervical cancer samples, but it did lead him to a closely related papillomavirus, ultimately named HPV-11. In 1983 zur Hausen published evidence that HPV-11 was present in three out of 24 cervical cancer samples he tested.
And now he and his team were on a roll. It became apparent that there were many different types of HPV. They continued their search and discovered HPV-16, which was detected in about half of cervical cancers, then HPV-18, present in around one in five cervical cancer samples.
It was becoming clear that infection with these two types was closely linked to cervical cancer – a discovery that eventually won zur Hausen a Nobel Prize.”

It became clear that there was a link between HPV and cervical cancer? Zero cases of cervical cancer for HPV-6? 3 out of 24 for HPV-11? About 50% for HPV-16? 1 in 5 for HPV-18? These statistics are what made it “become clear” that there was a link between HPV and cancer? It would be accurate to state that it was clear that they detected random DNA assumed to belong to newly “discovered” HPV’s but there definitely was no proof there was any “virus.” We get a little more clarity from Zur Hausen’s Nobel Prize write-up:
Nobel-Winning Discovery of HPV–Cervical Cancer Link
Already Having an Impact on Medicine
“But these innovations would not have been possible without the perseverance of 1 man, the scientist who proposed and then went on to prove the link between cervical cancer and HPV. The discovery caused quite a stir at the time — in the early 1980s — because the majority of experts did not believe that viruses could cause cancer, and the few who did were focusing on a different
virus altogether.
Against the Dogma of the Time
That scientist was Harald zur Hausen, MD, professor emeritus currently working at the German Cancer Research Center, in Heidelberg, and former scientific director of that Center. That discovery has just earned him half of the 2008 Nobel Prize for Physiology and Medicine, which he shared with 2 French scientists who discovered the human immunodeficiency virus (HIV). It is the latest and most prestigious of several prizes he has already won for this research, including the American Association of Cancer Research’s Award for Lifetime Achievement.
The Nobel citation said that Dr. zur Hausen went “against the current dogma of the time,” and his proposal for a role for HPV in cervical cancer flew in the face of prevailing views in the 1970s.
“My proposal was not very welcome at that time,” Dr. zur Hausen recalled in an interview recorded on nobelprize.org after the announcement. At that time, many researchers were focusing their attention on the herpes simplex virus; in fact, he delivered 1 of his first papers proposing HPV as the cause of cervical cancer at a meeting in Florida specifically scheduled to discuss herpes simplex research. “I was a lonely voice at that meeting,” he said.
It took some time to amass evidence to support the proposal. As the Nobel citation explains, Dr. zur Hausen assumed that the tumor cells, if they contained an oncogenic virus, should harbor viral DNA integrated in their genomes. But it took more than 10 years to show this, because the process was complicated by the fact that only parts of the viral DNA were integrated in the host genome.
The breakthrough came in the early 1980s, when Dr. zur Hausen and his team found novel HPV-DNA in cervical cancer biopsies, thus discovering the tumorigenic virus type HPV 16 in 1983. A year later, the team cloned HPV 16 and HPV 18 from patients with cervical cancer. The Nobel citation notes that the team made these clones available to the scientific community, and Dr. zur Hausen commented that they were “dispersed very freely throughout the world.” Ironically, others later patented and profited from this research.
Since then, HPV 16 and 18 have been consistently found in about 70% of cervical cancer biopsies throughout the world, the Nobel committee said. This research eventually led to the development of a vaccine against HPV 16 and HPV 18, which provides more than 95% protection from these infections. However, the committee was cautious in its predictions of the impact this will have, commenting that it “may reduce the need for surgery and the global burden of cervical cancer.”
Revolutionary Idea Took Time to Be Accepted
The finding that HPV caused cervical cancer was “absolutely revolutionary,” commented Maurie Markman MD, professor of gynecologic medical oncology at the University of Texas MD Anderson Cancer Center, in Houston, who acts as an editorial advisor to Medscape Oncology.
“This was the first time it was possible to unequivocally define an infectious agent as the cause of a cancer, demonstrate the process whereby the viral DNA affects the development of the cancer, and finally how a vaccine could potentially prevent the development of the cancer,” Dr. Markman commented.
So revolutionary was the idea that it took quite some time for the finding to be accepted among the scientific community, commented Attila Lorincz, PhD, professor of molecular epidemiology at the Wolfson Institute of Preventive Medicine, in the United Kingdom. Many experts could not believe that a virus could cause cancer, and were focusing instead on other environmental factors and
genetic predispositions, he said. “It was another 10 years before the majority of skeptics were silenced, and even a few years ago, there were still a few recalcitrant older medics and scientists.”

Zur Hausen ASSUMED that if there were “oncogenic viruses,” then “viral” DNA would be integrated into the tumor genomes. In other words, no need to find a “virus” only the fragments of DNA linked to it. However, the detection of “viral” RNA/DNA is essentially meaningless as shown recently by the disclaimers on “SARS-COV-2” PCR tests such as this:
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.”
https://www.google.com/url?sa=t&source=web&rct=j&url=https://www.fda.gov/media/134922/download&ved=2ahUKEwjniIzR5In3AhWELc0KHdreAPUQFnoECCoQAQ&usg=AOvVaw26_v3GqAn8Y9-F3w81SSQR
Zur Hausen found novel DNA, not a novel “virus.” Even with this discovery, his peers and even the Nobel Prize write-up were skeptical. Maybe they wanted to see actual purified/isolated HPV taken directly from a sick patient instead of random hybridized DNA fragments assumed to be a new “virus?” Maybe they needed to see proof that this “virus” was actually pathogenic? Finding random bits of DNA in some cervical cancer patients and claiming it is a new version of HPV and the cause of said cancer requires solid proof. This was not it.
In order to even attempt to say the DNA that Zur Hausen detected was “viral,” it would need to be shown that such a thing as a human “papillomavirus” exists before one can branch out hundreds of different versions of it and claim them as a cause of cervical cancer. This obvioulsy raises the question: Has HPV ever been properly purified and isolated directly from a sick patient and then proven pathogenic in a narural way?
The search for an answer to this question led me to a 1949 paper by Maurice Strauss, Henry Bunting, and Joseph Melnick. What the researchers did was collect warts from the hands and feet of children, grind the warts up, mix the resulting tissue crud with aluminum oxide and water, spin the mixture really fast for a while, and then take the supernatant and shadow cast it in chromium to view the sample under an electron microscope. The researchers then assumed whatever particles seen which resembled a “virus” were in fact one. In this case, the three researchers compared their choosen particles to those which were found in plants and claimed that they had discovered a “virus” as the particles resembled the plant “viruses.” Did Strauss, Bunting, and Melnick actually prove that these particles assumed to be HPV were an actual “virus?” No, as there were no attempts to prove pathogeniticity in the paper whatsoever. All the three researchers did was point at random particles and declare a “virus,” hence the “virus-like” particles in the title and the summary of the paper. Highlights below:
“Crystalline” Virus-Like Particles from Skin Papillomas Characterized by Intranuclear Inclusion Bodies.
“This is a report of the observation with the electron microscope of virus-like bodies that have been obtained from skin papillomas. These papillomas are characterized by the presence of intranuclear inclusion, bodies, and the elementary bodies obtained from them tend to be arranged in a crystalline-like pattern. Five such lesions were studied by electron microscopy.”
“The preparation of the material was the same in all instances. Half of each lesion was fixed in formalin for tissue sections while the remainder was promptly ground with alundum and distilled water and subjected to clarifying centrifugation of the supernatant fluid at 2,000 r.p.m. for 5 minutes followed by centrifugation of the resulting supernatant fluid at 6,000 r.p.m. for 15 to 45 minutes. Small drops of the 6,000 r.p.m. supernatant fluid and the resuspended sediment were placed on collodion mounts for electron microscopy. These were shadow cast with chromium at an angle of 1:7.

Examination with the electron microscope (RCA type EMU) revealed spherical particles most abundantly in the 6,000 r.p.m. sediment of the suspension frolm ithe papillomas showing intranuclear inclusion bodies. These particles were frequently arranged in crystalline-like clusters or layers with an average
diameter of 52 mp and a range of 50 to 53 mp (Fig. 1). Such an arrangement resembles that previuusly noted for crystalline plant viruses (Price, Williams, Wyckoff). When these particles were not in crystal-like array,
they averaged 68 mp in diameter with a range of 56 to 80 mp.”

“Search through the accumulated material of the laboratory of surgical pathology of the New Haven Hospital revealed 31 other skin lesions histologically similar to that of the inclusion body papillomas described above. The ages of these patients ranged from 2% to 68 years. There were also 158 typical verrucae from individuals 5 to 80 years of age.

Summary. Virus-like particles that tend to be arranged in a crystalline-like pattern have been observed by electron microscopy in a study of suspensions of 5 skin papillomas. Histological examination of the same tissues revealed intranuclear inclusion bodies and characteristic cytoplasmic masses in the cells of the hyperplastic epidermis. Thirty-one lesions with similar histological appearance were encountered along with 158 typical verrucae in a review of surgical pathological material.”
doi: 10.3181/00379727-72-17328.

In 1952, Melnick, Bunting, and Strauss were at it again with a follow-up study. Upon reading, it becomes obvious that even three years after their initial findings, the three researchers could still not claim HPV as a “virus:” They once again refer to HPV as “virus-like” particles. Upon examination again under EM, they referred to drawings and kodachromes to not confuse any masses with the chromatin (a substance within a chromosome consisting of protein, RNA, and DNA). They state that the crystalline structure was “probably” a “virus” primarily due to the similar pattern it formed with plant “viruses.” They admit that the material they examined was impure, the histopathological changes were APPARENTLY associated with “virus-like” particles, and that the eosinophilic inclusin body was PRESUMABLY indicative of the presence of a “virus.” Thus once again, no proof HPV is a “virus:”
ELECTRON MICROSCOPY OF VIRUSES OF HUMAN PAPILLOMA, MOLLUSCUM CONTAGIOSUM, AND VACCINIA, INCLUDING OBSERVATIONS ON THE FORMATION OF VIRUS WITHIN THE CELL
“This discussion will deal with electron microscopic studies of two lesions of human skin, papilloma and molluscum contagiosum. Both diseases are infectious, the etiological agents being filterable. Work on these viruses has been limited, however, in that the only known host is man. Our work on human papilloma was carried out in conventional fashion, i.e., isolation of cellular components by differential centrifugation and their examination in the electron microscope.”
“Material from the papillomas and from control specimens is ground with alundum and distilled water, centrifuged at 2,000 r.p.m. for five minutes, and the resulting supernatant fluid subjected to further centrifugation at 6,000 r.p.m. for 45 minutes. The sediment is resuspended in a small volume of distilled water (about 1 ml.). For electron microscopy a small drop is placed on a collodion screen and shadow-cast with chromium or palladium before examination. Although isolated particles may be found in all specimens, the particles are arranged in crystalline-like clusters with such regularity that this arrangement appears to be characteristic.”

“The histological appearance of the papillomas yielding virus-like particles is described in detail in a paper by Bunting and Strauss.”
“Absolute identification of the intranuclear inclusion bodies in the Feulgen preparations, to avoid confusion with chromatin masses, was insured by comparison with drawings and kodachromes of the same cells when previously stained with hematoxylin and eosin. Photomicrographs were taken at wave lengths of 2650 and 2800 k and evaluated visually.”

“The formations isolated from these papillomas constitute the first crystalline substance of this type obtained from any animal growth. This characteristic particle is probably virus in nature and responsible for the appearance and growth of the wart. In the past, spherical viruses have been found to yield such crystalline patterns. This has been particularly true of certain plant viruses and, on occasion, highly purified preparations of spherical bacteriophage have yielded similar patterns. However, the fact that relatively impure preparations of suspensions of these warts yield such patterns indicates the marked degree of attaction which these particles have for each other and their uniformity. The diameter of these particles, 52 mp, is the same order of magnitude as that found for the virus of the Shope rabbit papilloma.”
“The characteristic histopathological changes observed in these lesions, not seen in every common wart, are apparently associated with the presence of the virus-like particles described above. One would conclude that the normal development of the epidermal cells had been distorted to a greater degree than that occurring in simple hyperplasia. The eosinophilic intranuclear inclusion body presumably indicative of the presence of the virus, is small when it is first seen in the first or second layer of cells above the basal. It doubles in size by the time its identity is lost in the pyknotic nuclei of the parakeratotic stratum corneum.”
doi: 10.1111/j.1749-6632.1952.tb39990.x.

From the highlights taken from the above two papers, it is safe to say that HPV was never properly purified/isolated nor proven pathogenic. The researchers picked out the particles from impure samples that they assumed were the “virus” based on images from plant “viruses.” Now that we have the lack of a purified/isolated HPV “virus” out of the way, we can fast forward a few decades to 1983 in order to see what evidence Harald Zur Hausen was able to conjure up in order to claim that the never purified/isolated particles assumed to be HPV cause cervical cancer.
Upon reading the paper, you will find that no particles assumed to be a “virus” were ever found nor used in this study. All that was claimed is the detection of “novel” DNA from one cervical cancer sample which was then assumed to be a new HPV based on whether the DNA hybridized with other HPV sequences. Zur Hausen cloned this DNA in a phage and then used this synthetic creation to probe other cancer samples and found mixed results. The HPV DNA was seen in benign non-cancerous samples and was inconsistently found in related cancers. He also found a geographical difference between samples tested in Germany, where the DNA was found in 61% of the samples, to those in Kenya and Brazil where it was found in 34% of the samples. Interestingly, Zur Hausen admitted that the characterization of “papillomavirus” types was based exclusively on analysis of the DNA after molecular cloning and that many of the classified types had been identified only from tumor DNA carrying these genomes. He also admitted that the DNA had not yet been demonstrated in “papillomavirus” particles, thus confirming that the HPV strains only exist as DNA sequences and not as physical particles. To put a final nail in his own findings, Zur Hausen concluded that the regular presence of HPV DNA in genital cancer biopsy samples did not prove an etiological involvement of these “virus” infections. You can read the entire fictitious evidence for the claim that HPV causes cervical cancer below:
A papillomavirus DNA from a cervical carcinoma and its prevalence in cancer biopsy samples from different geographic regions
ABSTRACT DNA from one biopsy sample of invasive cancer of the cervix contained sequences hybridizing with human papillomavirus (HPV) type 11 DNA only under nonstringent conditions. This DNA was molecularly cloned in A phage. Under stringent conditions of hybridization it cross-hybridized to a minor extent (less than 0.1%) with HPV types 10, 14, and 15 and showed no homology with DNA of other human HPV types. We therefore propose to designate it tentatively as HPV 16. HPV 16 DNA was used as a probe to test additional cancer biopsy samples from cervical, vulval, and penile cancer, as well as benign genital warts (condylomata acuminata) and cervical dysplasias for the presence of homologous sequences. In 61.1% (11/18) of cervical cancer samples from German patients sequences were found hybridizing with HPV 16 DNA under conditions of high stringency. In contrast, only 34.8% (8/23) of cancer biopsy samples from Kenya and Brazil revealed this DNA. Vulval and penile cancer biopsy samples hybridized to 28.6% (2/7) or 25% (1/4), respectively. Only 2 out of 33 condylomata acuminata contained HPV 16 DNA. Both positive tumors harbored in addition HPV 6 or HPV 11 DNA. The data thus indicate that HPV 16 DNA prevails in malignant tumors, rendering an accidental contamination with papillomavirus DNA from adjacent papillomas rather unlikely. The rare presence in benign genital papillomas in addition to common genital papillomaviruses suggests a dependence of HPV 16 replication on helper virus.
There is increasing evidence that papillomaviruses may be involved in the etiology of certain cancers in animals and humans (for review see ref. 1). This accounts for carcinomas induced by the Shope papillomavirus in rabbits, fibrosarcomas and esophageal carcinomas induced by bovine papillomaviruses, ocular carcinomas in cattle and cutaneous carcinomas in sheep, and malignant conversions observed in epidermodysplasia verruciformis as well as occasionally in laryngeal papillomatosis. It is a common feature of malignant conversion after papillomavirus infection that it appears to require additional interaction with initiating events (2).
Human genital cancer reveals epidemiological characteristics of infectious events (3). Two virus groups have been found to play a role: herpes simplex viruses (4, 5) and human papillomaviruses (HPVs) (6, 7). Because our group consistently failed to detect herpes simplex DNA in cervical cancer biopsy specimens but provided evidence for initiator-like functions of these virus infections (ref. 8; unpublished data), we focused our interest on the persistence of papillomavirus DNA within genital tumors.
Two types of genital papillomavirus infections have been regularly demonstrated in genital papillomas (condylomata acuminata and atypical condylomata of the cervix): HPV 6 and HPV 11 (9-11). There may exist additional types within benign genital tumors (12).
Recently, three groups reported the presence of HPV DNA in some genital tumors: Green et al. (13) reported that 2 out of 31 cervical carcinomas and 2 out of 10 vulval carcinomas contained sequences related to a virus that probably represents HPV 10. Zachow et al. (14) reported DNA hybridizing with HPV 6 DNA under stringent conditions in two verrucous carcinomas of the vulva and one carcinoma in situ of the vulva. Under nonstringent conditions DNAs from one additional verrucous carcinoma and three carcinomas in situ of the vulva hybridized with DNA used by Green et al. (13) in their study. Gissmann et al. (refs. 10 and 15; unpublished data) detected DNA cross-reacting with or identical to HPV 6 or HPV 11 DNA in 6 Buschke-Lowenstein tumors (nonmetastasizing verrucous carcinomas) and in 5 out of 27 cervical cancer biopsy samples (3 of them representing invasive cancer and 2 carcinomas in situ). In the present study DNA hybridizing with HPV 11 under nonstringent conditions in one of these tumors was molecularly cloned and used as a probe for testing benign and malignant genital tumors for the presence of homologous sequences. The data reveal a startling prevalence of this DNA in malignant tumors and its very occasional presence in benign papillomas.
MATERIAL AND METHODS
Blot Hybridization of Cellular DNA. Tissue biopsy samples were kept frozen at -20’C. DNA was prepared by phenol/chloroform/isoamyl alcohol extraction as described (10). About 10 ug of tumor DNA was cleaved by using various restriction endonucleases, separated on agarose gels, and transferred onto nitrocellulose filters.
Hybridization was done in 0.75 M NaCl/0.075 M sodium citrate and various concentrations of formamide at 420C (10) with tRNA instead of calf thymus DNA as carrier. 32P-Labeled HPV DNA cloned in plasmid pBR322 was purified from the vector by electrophoresis prior to nick-translation. Filters were washed in 0.30 M NaCl/0.03 M sodium citrate/0. 1% sodium dodecyl sulfate at the respective hybridization temperature. For screening of tumor DNA, filters were hybridized under conditions of low stringency (400C below the melting temperature, tm), kept moist before and during exposure, rewashed under stringent conditions (200C below tm), and exposed again.
Cloning of Viral DNA. HPV DNA from a cervical carcinoma (laboratory code WV 2916) was cloned in bacteriophage A L 47 at the single BamHI site (11) and subcloned in pBR322.

RESULTS
By screening of a large number of cervical carcinomas under nonstringent conditions of hybridization (unpublished data) with HPV 11 DNA (11), one tumor (WV 2916) was found to harbor
papillomavirus sequences with an unusual Pst I cleavage pattern (Fig. 1) not detectable under stringent conditions. Further analysis of WV 2916 DNA (Fig. 2) showed a main band of 7.2 kilobase pairs (kb) after BamHI cleavage. This fragment was shortened by cleavage with EcoRl and migrated with the bulk of cellular DNA after HindIII cleavage (see also Fig. 3).

Additional bands of different length in lower concentrations were seen in each case (Fig. 2 Left, lanes b-d). Washing at conditions of high stringency (Fig. 2 Right) removed virtually all signals in WV2916 DNA compared to positive controls (Fig. 2, lanes a, e, and f). The construction of a genomic library and subsequent screening of plaques with 32P-labeled HPV 11 DNA under nonstringent conditions resulted in a number of recombinant phages containing the 7.2-kb fragment. Furthermore, several positive hybridizing plaques harbored DNA inserts of various lengths corresponding to the additional fragments seen in Fig. 2. The characterization of this DNA will be reported elsewhere.

The 7.2-kb fragment was subcloned in pBR322 and characterized with different restriction enzymes (unpublished data). Hybridization of WV 2916 DNA with labeled 7.2-kb DNA under stringent conditions (Fig. 3) resulted in a pattern similar to that seen in Fig. 2. However, the additional fragments were not detected with this probe, thus indicating heterogeneity of HPV sequences in this cervical carcinoma.
Blot hybridization of the 7.2-kb fragment with DNA from human papillomavirus types thus far characterized under stringent condition resulted in a positive reaction only with HPVs 10, 14, and 15 (G. Orth, personal communication) and one yet-unclassified isolate from an epidermodysplasia verruciformis patient (G. Orth, personal communication). The extent of cross-hybridization with these types was estimated to be less than 0.1%. It was therefore concluded that the 7.2-kb fragment from WV 2916 DNA represents another papillomavirus type, tentatively designated HPV 16.

HPV 16 DNA purified from the vector was used as probe for screening of a series of genital warts, dysplasias, and carcinomas in situ, as well as invasively growing genital carcinomas. Hybridization at low stringency followed by subsequent washing at high stringency after a first exposure permitted the detection of HPV 16-specific as well as more distantly related papillomavirus sequences in the same experiment (Figs. 4 and 5).
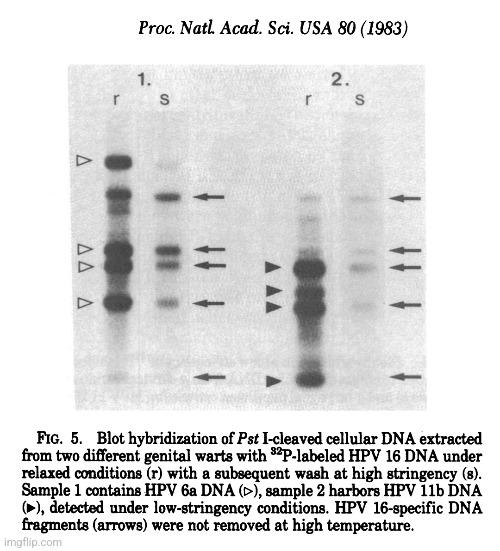
As shown in Table 1, 11 out of 18 cervical carcinomas from German patients contained HPV 16-specific sequences (Fig. 4). The DNA from one additional tumor hybridized only at conditions of low stringency and the DNA from another biopsy sample hybridized under stringent conditions with a DNA mixture of HPV 8, 9, 10, and 11 DNAs. The DNAs from only 8 out of 23 biopsy samples obtained from Africa and South America reacted under stringent conditions with HPV 16 DNA. The higher percentage of negative non-European tumors (65.2%) and those materials containing detectable concentrations of different papillomaviruses (8.7%) suggest that other virus types might be prevalent in tumors from patients in these areas.
HPV 16-specific and related sequences were also found in some dysplasias and carcinomas in situ of the cervix as well as in two vulval and one penile cancer (see Table 1). However, only 2 of 33 (6.1%) genital warts contained HPV 16 DNA as determined by the characteristic Pst I cleavage pattern (Fig. 5). Interestingly, these two tumors also harbored either HPV 6 or HPV 11 DNA.
DISCUSSION
Characterization of papillomavirus types is at present based exclusively on analysis of the DNA (16) after molecular cloning. Many of the classified types have been identified only from tumor DNA carrying these genomes and have not yet been demonstrated in papillomavirus particles (11). A low degree of base homology, detectable under hybridization conditions of reduced stringency (17), a similar gene organization (18, 19), and a nonintegrated episomal state (9) characterize the isolates obtained thus far.

Similar features are revealed by the papillomavirus DNA isolated directly from a biopsy sample of human invasive carcinoma of the cervix. This DNA hybridizes with HPV 6 or HPV 11 under nonstringent conditions and hybridized to a very low degree (less than 0.1%) with HPV 10, 14, 15, and a yet-un-classified type isolated from a epidermodysplasia verruciformis patient (G. Orth, personal communication) at high stringency, whereas no positive reaction was obtained with the other virus types under those conditions. A comparison with HPV 7 DNA was not possible because cloned DNA of this type is not yet available. The fact that up to now this papillomavirus DNA has been found to occur exclusively in butcher’s hand warts (20, 21) renders identity with the cervical papillomavirus DNA rather unlikely. The isolate described here is therefore tentatively designated as HPV 16. HPV 16 DNA exists in an extrachromosomal state in the tumor (unpublished data). The circular molecules, however, seem to be present in multimeric forms.
The presence of this DNA in more than 60% of cervical cancer biopsy specimens from German patients and its absence from most benign papillomas from the same region is a startling observation. It reveals a remarkable specificity of HPV 16 infections for malignant tissue. This renders an accidental contamination from adjacent papilloma tissue rather unlikely. The presence of this DNA in 2 out of 33 condylomata acuminata in addition to much larger quantities of either HPV 6 or HPV 11 could provide a clue for the peculiar distribution of HPV 16 DNA. Although HPV 16 exists solely as circular molecules of monomeric length in these lesions (unpublished data), one is tempted to speculate that HPV 16 DNA is defective and requires complementation by additional papillomavirus types for particle encapsidation and infectivity. This of course has to be substantiated by further experimentation.
The DNA showed some heterogeneity in cancer tissue, suggesting either the existence of various subtypes or genomic rearrangements during cancer development.
There seems to exist some geographic difference in the incidence of HPV 16 infections in human genital cancer. Only 34.8% of cervical cancer biopsy specimens obtained from Kenya and Brazil contained cross-hybridizing sequences. This may reflect the prevalence of other papillomavirus types in these regions. Indeed, at least three additional types have been demonstrated within human genital cancer biopsy samples: HPV 6 in Buschke-Lowenstein tumors or verrucous carcinomas of vulva and penis (10, 14), virus DNA probably identical with HPV 10 in 2 out of 31 cervical cancers and in 2 out of 10 vulval cancers (13), and HPV 11 DNA in a few cervical cancers (15). It is thus apparent that different types of papillomaviruses can be found in genital squamous cell carcinomas. This is further underlined by this study, which has revealed additional positive tumors by hybridizing under conditions of low stringency with other types of HPV DNA. At present, the total percentage of positive cervical cancer biopsy samples (German cases) amounts to 72%. We do expect that characterization of further types of HPV will increase the percentage of positive tumors.
The regular presence of HPV DNA in genital cancer biopsy samples does not per se prove an etiological involvement of these virus infections, although the apparent cancer specificity of HPV 16 is suggestive of such a role. Their biological significance as well as the proposed interaction with initiating events (2) certainly requires further investigation.”
https://doi.org/10.1073/pnas.80.12.3812

In Summary:
- Harald Zur Hausen began his quest by looking for “viruses” in human genital warts, leading to the discovery of a new type of “papillomavirus,” which he called HPV-6
- Much to his disappointment, his team couldn’t find HPV-6 in any cervical cancer samples, but it did lead him to a closely related “papillomavirus,” ultimately named HPV-11
- In 1983 zur Hausen published evidence that HPV-11 was present in three out of 24 cervical cancer samples he tested
- He continued his search and discovered HPV-16, which was detected in about half of cervical cancers, then HPV-18, present in around one in five cervical cancer samples
- The discovery caused quite a stir at the time — in the early 1980s — because the majority of experts did not believe that “viruses” could cause cancer
- That discovery earned him half of the 2008 Nobel Prize for Physiology and Medicine, which he shared with 2 French scientists who discovered the human immunodeficiency “virus” (HIV) (should be all one needs to know right there)
- The Nobel citation said that Dr. zur Hausen went “against the current dogma of the time,” and his proposal for a role for HPV in cervical cancer flew in the face of prevailing views in the 1970s
- “My proposal was not very welcome at that time,” Harald zur Hausen recalled in an interview
- At that time, many researchers were focusing their attention on the herpes simplex “virus”
- It took some time to amass evidence to support the proposal
- Harald zur Hausen assumed that the tumor cells, if they contained an oncogenic “virus,” should harbor “viral” DNA integrated in their genomes
- But it took more than 10 years to show this, because the process was complicated by the fact that only parts of the “viral” DNA were integrated in the host genome
- His team found novel HPV-DNA (i.e. not a “virus” but its assumed DNA) in cervical cancer biopsies, thus “discovering” the tumorigenic “virus” type HPV 16 in 1983
- A year later, the team cloned HPV 16 and HPV 18 from patients with cervical cancer (where were HPV 16 and 18 ever purified and isolated?)
- HPV 16 and 18 have been consistently found in about 70% of cervical cancer biopsies throughout the world (i.e. they have found DNA in biopsies assumed but never proven to be “viral”)
- The Nobel committee was cautious in its predictions of the impact the vaccine will have, commenting that it “may reduce the need for surgery and the global burden of cervical cancer.”
- “This was the first time it was possible to unequivocally define an infectious agent as the cause of a cancer, demonstrate the process whereby the viral DNA affects the development of the cancer, and finally how a vaccine could potentially prevent the development of the cancer,” Dr. Markman commented
- So revolutionary was the idea that it took quite some time for the finding to be accepted among the scientific community
- Many experts could not believe that a “virus” could cause cancer, and were focusing instead on other environmental factors and genetic predispositions
- “It was another 10 years before the majority of skeptics were silenced, and even a few years ago, there were still a few recalcitrant older medics and scientists.” (silenced does not mean proven wrong)

- A 1949 paper by Maurice Strauss, Henry Bunting, and Joseph Melnick reported on the observation with the electron microscope of “virus-like” bodies that were obtained from skin papillomas
- Five such lesions were studied by electron microscopy
- Half of each lesion was fixed in formalin for tissue sections while the remainder was promptly ground with alundum and distilled water and subjected to clarifying centrifugation of the supernatant fluid at 2,000 r.p.m. for 5 minutes followed by centrifugation of the resulting supernatant fluid at 6,000 r.p.m. for 15 to 45 minutes
- These were shadow cast with chromium at an angle of 1:7
- The resulting arrangements resembled that previously noted for crystalline plant “viruses”
- Search through the accumulated material of the laboratory of surgical pathology of the New Haven Hospital revealed 31 other skin lesions histologically similar to that of the inclusion body papillomas described above
- They concluded that “virus-like” particles that tend to be arranged in a crystalline-like pattern were observed by electron microscopy in a study of suspensions of 5 skin papillomas

- In their 1953 paper, Maurice Strauss, Henry Bunting, and Joseph Melnick state that their work on human papilloma was carried out in conventional fashion, i.e., isolation of cellular components (i.e. not “viruses) by differential centrifugation and their examination in the electron microscope
- Again we see material from the papillomas and from control specimens is ground with alundum and distilled water, centrifuged at 2,000 r.p.m. for five minutes, and the resulting supernatant fluid subjected to further centrifugation at 6,000 r.p.m. for 45 minutes
- The sediment is resuspended in a small volume of distilled water (about 1 ml.)
- For electron microscopy a small drop is placed on a collodion screen and shadow-cast with chromium or palladium before examination
- Although isolated particles may be found in all specimens, the particles are arranged in crystalline-like clusters with such regularity that this arrangement appeared to be characteristic
- In other words, these were not purified/isolated samples they are looking at
- The histological appearance of the papillomas yielding “virus-like” particles was described in detail in a paper by Bunting and Strauss
- Absolute identification of the intranuclear inclusion bodies in the Feulgen preparations, to avoid confusion with chromatin masses, was insured by comparison with drawings and kodachromes of the same cells when previously stained with hematoxylin and eosin
- If there was a potential for confusion with chromatin masses, this is further evidence the sample contained more than the assumed “virus” particles
- Photomicrographs were taken at wave lengths of 2650 and 2800 k and evaluated visually
- They believed that this characteristic particle was probably “virus” in nature and responsible for the appearance and growth of the wart
- They claim that in the past, spherical “viruses” have been found to yield such crystalline patterns (except the same lack of purification, isolation, and proof of pathogenicity can be applied to these particles as well)
- The fact that relatively impure preparations of suspensions of these warts yield such patterns indicated the marked degree of attaction which these particles have for each other and their uniformity (i.e. further admittance the particles representing HPV were picked out from an unpurified source)
- The characteristic histopathological changes observed in these lesions, not seen in every common wart, were apparently associated with the presence of the “virus-like” particles
- The eosinophilic intranuclear inclusion body was presumably indicative of the presence of the “virus”
- This study amounts to the three researchers picking a representative particle from impure sources and assigning histological effects to the particles without proof

- DNA from one biopsy sample of invasive cancer of the cervix contained sequences hybridizing with human papillomavirus (HPV) type 11 DNA only under nonstringent conditions
- Under stringent conditions of hybridization it cross-hybridized to a minor extent (less than 0.1%) with HPV types 10, 14, and 15 and showed no homology with DNA of other human HPV types
- HPV 16 DNA was used as a probe to test additional cancer biopsy samples
- Only 2 out of 33 condylomata acuminata contained HPV 16 DNA
- Both positive tumors harbored in addition HPV 6 or HPV 11 DNA
- The data thus indicate that HPV 16 DNA prevails in malignant tumors, rendering an accidental contamination with papillomavirus DNA from adjacent papillomas rather unlikely (i.e not a purified sample)
- The rare presence in benign genital papillomas (i.e. non-canverous) in addition to common genital papillomaviruses suggested a dependence of HPV 16 replication on helper “virus”
- Zur Hausen claimed that there was increasing evidence that “papillomaviruses” may be involved in the etiology of certain cancers in animals and humans
- It is a common feature of malignant conversion after “papillomavirus” infection that it appears to require additional interaction with initiating events
- Two “virus” groups were said to have been found to play a role in cancer: herpes simplex “viruses” and human “papillomaviruses” (HPVs)
- Zur Hausen’s group consistently failed to detect herpes simplex DNA in cervical cancer biopsy specimens (perhaps because the DNA has never been proven to come from a purified/isolated herpes simplex “virus?”)
- Thus they focused their interest on the persistence of “papillomavirus” DNA (also never proven to come from purified/isolated “virus” particles) within genital tumors
- There may exist additional types of HPV within benign genital tumors
- Green et al. reported that 2 out of 31 cervical carcinomas and 2 out of 10 vulval carcinomas contained sequences related to a “virus” that probably represents HPV 10
- Gissmann et al. detected DNA cross-reacting with or identical to HPV 6 or HPV 11 DNA in 6 Buschke-Lowenstein tumors (nonmetastasizing verrucous carcinomas) and in 5 out of 27 cervical cancer biopsy samples
- Zur Hausen stated that in his study, DNA hybridizing with HPV 11 under non-stringent conditions in one of these tumors was molecularly cloned and used as a probe for testing benign and malignant genital tumors for the presence of homologous sequences
- The data reveal a startling prevalence of this DNA in malignant tumors and its very occasional presence in benign papillomas (i.e. the DNA was found in non-cancerous tumors as well)
- DNA was prepared by phenol/chloroform/isoamyl alcohol extraction as described
- About 10 ug of tumor DNA was cleaved by using various restriction endonucleases, separated on agarose gels, and transferred onto nitrocellulose filters
- Hybridization was done in 0.75 M NaCl/0.075 M sodium citrate and various concentrations of formamide at 420C (10) with tRNA instead of calf thymus DNA as carrier
- 32P-Labeled HPV DNA cloned in plasmid pBR322 was purified from the vector by electrophoresis prior to nick-translation
- Filters were washed in 0.30 M NaCl/0.03 M sodium citrate/0. 1% sodium dodecyl sulfate at the respective hybridization temperature
- HPV DNA from a cervical carcinoma (laboratory code WV 2916) was cloned in bacteriophage A L 47 at the single BamHI site (11) and subcloned in pBR322 (commonly used plasmid cloning vector in E. coli)
- By screening of a large number of cervical carcinomas under nonstringent conditions of hybridization (unpublished data) with HPV 11 DNA (11), one tumor (WV 2916) was found to harbor papillomavirus sequences with an unusual Pst I cleavage pattern not detectable under stringent conditions
- The construction of a genomic library and subsequent screening of plaques with 32P-labeled HPV 11 DNA under nonstringent conditions resulted in a number of recombinant (various sources of combined DNA) phages containing the 7.2-kb fragment
- Side Note: Recombinant DNA (rDNA) molecules are DNA molecules formed by laboratory methods of genetic recombination (such as molecular cloning) that bring together genetic material from multiple sources, creating sequences that would not otherwise be found in the genome.
- https://en.m.wikipedia.org/wiki/Recombinant_DNA
- The characterization of this DNA was not reported in this paper
- The 7.2-kb fragment was subcloned in pBR322 and characterized with different restriction enzymes (unpublished data)
- The additional fragments were not detected with this probe, thus indicating heterogeneity (i.e. not the same) of HPV sequences in this cervical carcinoma
- Blot hybridization of the 7.2-kb fragment with DNA from human “papillomavirus” types thus far characterized under stringent condition resulted in a positive reaction only with HPVs 10, 14, and 15 (G. Orth, personal communication) and one yet-unclassified isolate from an epidermodysplasia verruciformis patient (G. Orth, personal communication) (in other words, once again unpublished data)
- It was therefore concluded that the 7.2-kb fragment from WV 2916 DNA represents another “papillomavirus” type, tentatively designated HPV 16
- HPV 16 DNA purified from the vector was used as probe for screening of a series of genital warts, dysplasias, and carcinomas in situ, as well as invasively growing genital carcinoma
- In other words, they used an unknown DNA sequence they created and assumed was a new HPV to screen cancer samples
- 11 out of 18 cervical carcinomas from German patients contained HPV 16-specific sequences
- The DNAs from only 8 out of 23 biopsy samples obtained from Africa and South America reacted under stringent conditions with HPV 16 DNA
- The higher percentage of negative non-European tumors (65.2%) and those materials containing detectable concentrations of different papillomaviruses (8.7%) suggest that other “virus” types might be prevalent in tumors from patients in these areas
- Only 2 of 33 (6.1%) genital warts contained HPV 16 DNA as determined by the characteristic Pst I cleavage pattern
- Interestingly, those two tumors also harbored either HPV 6 or HPV 11 DNA
- Characterization of “papillomavirus” types was based exclusively on analysis of the DNA after molecular cloning
- Many of the classified types had been identified only from tumor DNA carrying these genomes and had not yet been demonstrated in “papillomavirus” particles
- In other words, everything relating to HPV is based on random DNA that can not be linked to “virus” particles
- HPV 16 DNA exists in an extrachromosomal state in the tumor (unpublished data)
- Zur Hausen stated that the presence of this DNA in more than 60% (i.e. not all cases) of cervical cancer biopsy specimens from German patients and its absence from most benign papillomas (i.e. it is found in non-cancerous cases) from the same region was a startling observation
- This renders an accidental contamination from adjacent papilloma tissue rather unlikely (once again, unpurified)
- Although HPV 16 exists solely as circular molecules of monomeric length in these lesions (unpublished data), one is tempted to speculate that HPV 16 DNA is defective and requires complementation by additional “papillomavirus” types for particle encapsidation and infectivity
- The DNA showed some heterogeneity (i.e. not the same) in cancer tissue, suggesting either the existence of various subtypes or genomic rearrangements during cancer development
- Zur Hausen admitted that there existed some geographic difference in the incidence of HPV 16 infections in human genital cancer as only 34.8% of cervical cancer biopsy specimens obtained from Kenya and Brazil contained cross-hybridizing sequences
- He stated that this may reflect the prevalence of other “papillomavirus” types in these regions:
- HPV 6 in Buschke-Lowenstein tumors or verrucous carcinomas of vulva and penis
- “Virus” DNA probably identical with HPV 10 in 2 out of 31 cervical cancers and in 2 out of 10 vulval cancers
- HPV 11 DNA in a few cervical cancers
- The total percentage of positive cervical cancer biopsy samples (German cases) amounted to 72% (total of all HPV detected, not just HPV 16)
- He expected that characterization of further types of HPV will increase the percentage of positive tumors
- Zur Hausen concluded that the regular presence of HPV DNA in genital cancer biopsy samples does not per se prove an etiological involvement of these “virus” infections, although the apparent cancer specificity of HPV 16 is suggestive of such a role
- He stated that their biological significance as well as the proposed interaction with initiating events certainly required further investigation

Zur Hausen’s paper is a microcosm of what is wrong with virology. He assumed a “virus” can cause cervical cancer. He assumed it was HPV. Even though the DNA he found cross-hybridized with HPV 10, 14, and 15 less than 0.1% and shared no homolgy with any other HPV, he assumed he had discovered HPV-16. When he used the HPV-16 DNA to probe for evidence, he could only find it in some (not all) cases of cervical cancer which varied wildly by geographical location and yet he still assumed it was the cause of the cancer.
When the researcher who assumes all of these things as true then admits in his own paper that:
- Characterization of “papillomavirus” types was based exclusively on analysis of the DNA after molecular cloning
- Many of the classified types had been identified only from tumor DNA carrying these genomes and had not yet been demonstrated in “papillomavirus” particles
- Finding the DNA said to be associated with HPV does not prove that HPV causes the cancer it has been associated with
- Further investigation into the biological significance as well as the proposed interaction with initiating events was required
There are some pretty big problems with said evidence.
All that can be claimed is the identification of random DNA that is assumed to be “viral” without any purified and isolated physical particles backing it up. Perhaps this is why Harald Zur Hausen’s contemporaries were skeptical of his findings and the link between cancer and “viruses.” That is, until they were silenced.


Yet again a giant mess of begging the question. Thanks for this great deconstruction of the umpteenth virus delusion. Guillain Barré Syndrome is one of the “side effects” of the injection they give to young girls worldwide and they’re now pushing the shot to boys as well. I’ll be sharing this article widely.
LikeLiked by 2 people
Thanks! The HPV vaccine is one of the worst and most dangerous vaccines. I hope people realize the scam that this was all built upon and reject it.
LikeLiked by 1 person
I remember this whole ‘episode’ playing out in the media. As soon as I started to see such ‘reports’ on the news I said to my FOO, now watch, within 2 months they’ll be promoting the vaccine along with these so-called studies on the news. Sure enough! But then they still believe it all. If I thought your excellent work would change their minds I’d share it, but until it comes out of the mouth of a reporter on CNN, they won’t believe it. Not to undermine your work AT ALL, it’s awesome, and it will most certainly change some minds, who will hopefully then go on to work at CNN—hehe—but I won’t hold my breath.
LikeLiked by 1 person
Thanks! I’m well aware that many will not take my research seriously. For some, it won’t matter if the information were to come from a virologist as in the case of Dr. Lanka. There are sadly people who just don’t want to be convinced. They would rather remain plugged in to the matrix. I’m here for those who are willing to take those first initial steps. 😉
LikeLiked by 1 person
The vaccine enigma continues. After about 100 years of vaccines and thousands of miracle drugs, why is man still dying of sickness and disease before his time? Our toxic planet is killing us and all big pharma can do is speed up the process with it’s poisons.
LikeLiked by 1 person
Exactly. Our “healthcare” industry is contributing to our decline rather than preventing it.
LikeLike
I was expecting the so-called “research” to be a whole lotta assumption, DNA-manipulation and fuzzy EM images but this is really over-the-top. Whenever i read about HPV, or course I think of Gardasil. Over the years reading from RFK Jr and watching some of his presentations, I know this jab is one of the most posionous of them all. As of Oct. 2021, there were 12 Gardasil lawsuits filed alleging Merck knew HPV vaccine was ‘Defective and Unreasonably Dangerous’.
LikeLiked by 1 person
It’s sad so many girls and boys are being injected with dangerous toxins based on nothing. I really wish more people read and understood the papers so that they could see the lack of scientific evidence for themselves.
LikeLiked by 1 person
Mr Mike first off I am very grateful for your priceless and relentless efforts in uncovering the greatest deception of our time. So regarding any type of cancer I am very much certain of the fact that far from an imaginary virus as a culprit, there is definitely much is going on inside our body. And under such circumstances maybe don’t you think works like german new medicine of Dr. Hamer is worth studying and giving serious heed for?
LikeLiked by 1 person
Thanks for the kind words! I was just recently asked this by another person and I will share some of my response here:
“While I understand where you are coming from, I have yet to see any solid scientific evidence for GNM. However, I will not discount it as I have not really delved into GNM in great detail. The problem I have is it seems GNM swings too far into the mental aspect while discounting the accumulative effects of physical stressors. There are many physical. factors which lead to disease such as air pollution, non-organic pesticide-laden foods, unclean fluoridated/chlorinated water, pharmaceuticals and vaccines, alcohol and drug use, lack of exercise and sleep, EMF’s and other radiation, etc. I put equal weight on all of these along with emotional stressors. In my opinion, it is a combination of physical and mental toxicity which leads to disease.
There are so many factors that go into disease. It is a complicated process. To claim it is as simple as a brain-directed organ adaptation process seems to be missing the bigger picture. There is no one cause or factor leading to disease but many complex ones. We may never understand how it all works. However, if we take care of both our physical and mental health and maintain balance, we will live long healthy lives.”
Now, like I said, I have only scratched the surface of GNM as I’ve been busy looking at other things. I would never discourage anyone from looking into it and researching the subject for themselves. For myself, I have not seen much in the way of scientific validation for GNM and what I have seen is more in terms of testimonials. I do hope to look into it someday soon. At the moment, I still believe health is finding a balance between physical and emotional stressors. We may never truly understand exactly how it all works. However, I do feel if we maintain balance and put equal weight on the physical and mental factors which can lead to disease, we have the best chance of staying healthy.
LikeLiked by 1 person
I am more of positive with everything you just said. But to add something of great importance is the fact that what the conventional medicine dub the term as “placebo effect”, if we try to assess it by as many principles/methods as the materialistic science would allow us to, I am pretty sure we only reach dead ends of explanation. So pursuing alternatives for atleast making any sense out of it, if not at all providing outright conclusive explanations is of great concern we should all take.
LikeLiked by 1 person
The placebo effect is easily explained by the fact that the body recognizes that “when there’s emotional pattern X, our cleaning processes tend to get interfered with soon after” – the emotional pattern of the person taking a drug, feeling confident, etc. – “so we as well give up on these cleaning processes until this blows over.”
I put English phrasing on it, but it’s a simple primed physiological response pattern like any other, such as a taste aversion reaction after eating rotten food.
Our minds may not understand much of what our body is trying to tell us anymore (until we get back in touch with it), but our bodies certainly understand the emotional communications from the mind.
LikeLiked by 1 person
The nocebo effect is likewise, “We’re getting the emotional pattern that we’re about to get poisoned; Start up the detox machinery!”
So symptoms can come, as usually there are other things to clean anyway and the emotion of having been poisoned is often enough to tip the scales in the body’s decision-making process.
All these “ultra-mysterious phenomena” are easy to understand when you realize the body creates most of what medicine calls “symptoms” intelligently and deliberately to clean and repair itself.
LikeLiked by 1 person
I think the nocebo effect is a majorly overlooked component to all of this. There has been a well-orchestrated fear campaign that drilled the idea of “unusual” symptoms (such as Anosmia) into the collective consciousness and people are now hyper aware of these symptoms and can manifest them through fear. This is why I believe fear is the real “virus.”
LikeLike
The main reason on why I put the “placebo effect” matter into this discussion in the first place is to enlighten the very fact that according to mainstream medicine which looks the body as nothin more than just piece of inert material that goes in quite predictable and predetermined way, phenomena such as “placebo” and “nocebo” are indeed anomalies in the scope of this doctrine. The key elements as belief, anticipation or expectation without which we can barely make any sense out of such anomalies, are attributed to mind-body(Psycho-Soma) interaction, and are not definitely a byproduct of some exogenous factor rendering the inert body to produce some effects.
And likewise if only we happen to embrace the possibility that with almost most, if not all, of what we call diseases, body malfunctions, and disorders of some kind there might be subtle and a complex link between our beliefs, expectations and psychological status( mind) and the signs, symptoms,and biochemical fluctuations that are displayed (body). Afterall lookin at our body and how it works is as good as looking at the tip of the iceberg.
LikeLiked by 1 person
Yes, there is much we do not know and/or understand but it seems very clear that the mind and ones perceptions/beliefs heavily influence health. I believe in order to achieve optimal health, both physical and mental factors/stressors must be dealt with and be balanced. Yin/Yang so to speak. It is unwise to only look at one side while ignoring the other.
LikeLike
I hope this finds you I am very curious. I do not do vaccines. They are toxic bull. But what I don’t understand is warts and herpes. So please explain. If they are not a virus what are they ? Because they. Are contagious. I know some who say there is no germ it’s your immune system. But with these “germs “ whatever they are. Do come back. And yes it is based on immune system. It can beat it and get better. The warts normally don’t go away. You must kill it. And the herpes. They always come back when the immune system is down. So what is it ?? It’s hiding inside you and comes out. I just don’t understand. Please help.
LikeLike
Hi Aliveandfree,
Many of these “sexually transmitted diseases” are brought about by friction during intercourse, the lubricants and toys used, allergies to latex in condoms and spermicides, etc. They are either injuries and/or detoxification processes that are flusing out toxins through the skin. The symptoms can also be brought about by similar environmental toxins as well as drug use, which creates the appearance that one person passed something on to another person.
You may find these articles on syphilis helpful as they deal with eruptions of the skin blamed on sexual acts:
https://mikestone.substack.com/p/the-syphilis-scam
https://mikestone.substack.com/p/the-syphilis-scam-ricords-ruse
https://mikestone.substack.com/p/the-syphilis-scam-imitation-game
LikeLike