
Most of the known viral diseases were excluded and the infectious agent was shown to be a hitherto unknown virus with many peculiar characteristics: it infects guinea pigs but not adult mice and is larger than known viruses and of different shape.
Preface to Marburg Virus Disease by G. A. MARTINI • R. SIEGERT
If you’ve been paying attention to the mainstream media for some reason, you’re probably well aware of the re-emergence of many different “viruses” seemingly sprouting up around the world over the last few months. We’ve seen the oddly accurate prediction of the monkeypox in May 2022, the threats of oscure “viruses” such as nipah/langya, hantavirus, strawberry hepatitis A, the tomato flu, and the apparent reappearance of polio. One of the other lesser known “viruses” currently making the rounds in the media is known as the Marburg “virus.” While it may not be as scary sounding to those who are unfamiliar with it, the “virus” has a close relative whose name may be enough to strike fear into the hearts of the ignorant. For those who do not know, the Marburg “virus” is the original incarnation of the Ebola “virus.” My guess is you may be more familiar with the latter of the two.

In recent weeks, there have been reports of the Marburg “virus” making its presence felt in Ghana, a place which has never reported a case of the deadly “virus” before. Sadly, not only did Ghana report its first Marburg case early July 2022, they also reported their first deaths associated with the disease:
“An outbreak of Marburg fever has been detected in Ghana, whereas West Africa had been free of cases except for one case in Guinea in 2021. Currently, 98 people are considered contacts and are in isolation. No cases of Marburg fever have yet been detected among these contact cases.
So far two unrelated men have had Marburg fever. Presenting symptoms such as diarrhea, fever, nausea and vomiting, the two men, aged 26 and 51, have both died.”
https://unric.org/en/marburg-virus-disease-origins-and-symptoms/
If you listen to the mainstream media, you may be convinced to believe that the Marburg “virus” is a “highly contagious, highly virulent” and deadly disease ready to burst forth and become the next epidemic in need of fearing:
The life-threatening virus is highly contagious, and has no known cure or approved vaccine.
https://www.usatoday.com/story/news/health/2022/07/28/marburg-virus-disease-outbreak-symptoms-treatment/10173445002/
The WHO calls the disease “epidemic-prone,” meaning that it can spread easily between people if not prevented.
https://www.healthline.com/health-news/could-the-marburg-virus-start-another-outbreak-what-we-know
Marburg virus disease is a highly virulent disease that causes haemorrhagic fever, with a fatality ratio of up to 88%. It is in the same family as the virus that causes Ebola virus disease.
https://www.who.int/health-topics/marburg-virus-disease#tab=tab_1
Although MVD is uncommon, MARV has the potential to cause epidemics with significant case fatality rates.
https://www.ecdc.europa.eu/en/infectious-disease-topics/z-disease-list/ebola-virus-disease/facts/factsheet-about-marburg-virus
However, looking into the Marburg “virus” outbreaks tells an entirely different story. This is only the second reported outbreak of the Marburg “virus” in West Africa, a place where it was unheard of before. The first appearance in this region of what is considered a highly contagious “virus” said to spread through contact with bodily fluids was a single case reported in Guinea last year. Similar to the recent monkeypox outbreak, the patients diagnosed with Marburg in Ghana had no relation to each other, no travel history to an endemic country, nor any contact with any animals said to carry the “virus.” Both were farmers who reported non-specific symptoms such as diarrhea, fever, nausea and vomiting. Sadly, they both succumbed to their symptoms after treatment at the hospital. The final toll of this outbreak of the “highly contagious virus” was limited to four people.
How did a “highly contagious virus,” which has never been seen in West Africa before, make its way to that part of the continent when those infected had no history of travel to an area where the “virus” is said to be endemic? How did this deadly “virus” only infect one person in Guinea in 2021 and only 4 in Ghana in 2022 if it is highly virulent and contagious? In fact, in the vast majority of its history, the Marburg “virus” has shown that it is anything but “highly contagious,” with the highest outbreak occurring in Angola in 2004 with only 252 cases. If we are to go by the CDC’s own data, there have only been 475 total cases of this “highly contagious virus” worldwide since its discovery in 1967. Those statistics do not seem to jibe with the definition of a “epidemic-prone highly contagious, highly virulent virus.”
So what is the story behind the Marburg “virus?” When and how did this dangerous pathogen burst onto the scene? What new symptoms of disease originally prompted the search for a novel etiological agent? What methods, if any, were employed in order to purify, isolate, and characterize the particles assumed to be the “virus?” Let’s see what we can uncover about the first “virus” discovered in the Filoviridae family.
According to the CDC, the Marburg “virus,” was discovered in 1967 after an outbreak of symptoms commonly associated with hemorrhagic fever occurred among laboratory workers conducting research who had come in contact with African green monkeys. It is one of seven species of “filovirus,” with the other six belonging to separate versions of the Ebola “virus.” The symptoms of the disease associated with the Marburg “virus” are non-specific and overlap with many different diseases, such as malaria, typhoid fever, or dengue and/or any of the “viral” hemorrhagic fevers that may be endemic to a specific area. This obviously makes clinical diagnosis difficult (i.e. impossible) due to the similarities between the diseases. In other words, there is nothing new nor specific regarding the Marburg “virus” as it is just another in a long chain of names given to the same symptoms of disease:
“Marburg virus disease (MVD) is a rare but severe hemorrhagic fever which affects both people and non-human primates. MVD is caused by the Marburg virus, a genetically unique zoonotic (or, animal-borne) RNA virus of the filovirus family. The six species of Ebola virus are the only other known members of the filovirus family.
Marburg virus was first recognized in 1967, when outbreaks of hemorrhagic fever occurred simultaneously in laboratories in Marburg and Frankfurt, Germany and in Belgrade, Yugoslavia (now Serbia). Thirty-one people became ill, initially laboratory workers followed by several medical personnel and family members who had cared for them. Seven deaths were reported. The first people infected had been exposed to Ugandan imported African green monkeys or their tissues while conducting research. One additional case was diagnosed retrospectively.”
“Clinical diagnosis of Marburg virus disease (MVD) can be difficult. Many of the signs and symptoms of MVD are similar to other infectious diseases (such as malaria, typhoid fever, or dengue) or viral hemorrhagic fevers that may be endemic in the area (such as Lassa fever or Ebola). This is especially true if only a single case is involved.”
https://www.cdc.gov/vhf/marburg/index.html

We can learn a lot about the “discovery” of this new “filovirus” from the writings of Werner Slenczka, a man who self-identifies as an expert in “filoviruses” as he was intimately involved with their origin. Dr. Slenczka is an associate professor at the Institute of Virology who helped identify the filament-like particles claimed to be the “virus” by way of electron microscopy. He wrote a few papers detailing what occured throughout the “discovery” process and offered some rather interesting revelations.
The first excerpts presented here are from a paper he published on the Marburg “virus” in 2007, 40 years after it was first identified. According to Slenczka, the first people “infected” with the “virus” in August of 1967 were treated in their own homes for up to 10 days. The symptoms were not alarming at first but progressively became worse as undisclosed treatments were administered. It was initially thought that the patients were suffering from typhoid fever or dysentery. As the symptoms became worse, the patients were admitted to the hospital. Of the 7 patients who became hemorrhagic, 5 eventually succumbed to their illness, some as soon as one day after admission. Cases of the new “virus” as well as estimates for the incubation period were eventually determined retrospectively. Interestingly, one of the patients with severe illness who was never hospitalized recovered completely on his own. Contrary to the claims of the mainstream media today, it was eventually decided at the time that the “virus” was not highly contagious as there were only a few secondary cases, no tertiary infections, and no new cases after the initial “outbreak.”
In mid-September of 1967, experiments with Guinea pigs were started in order to determine the cause of the disease. The researchers serially passaged toxic goo between the Guinea pigs and created “similar” symptoms to the human disease after later passages, thus concluding that they had obtained a filterable “virus,” even though they were unable to obtain any electron microscopy images of the “virus.” Guinea pig spleen and liver tissues were examined by Slenczka using indirect fluorescence antibody testing and it was found that there were intracytoplasmic intrusions in the Guinea pigs, but not the humans. This method was used to select the blood of the “infected” animals which were then used for electron microscopy examination using a newly developed technique by the lead researcher. They subsequently “discovered” the “virus” in the animals (but not the humans) in November of 1967, nearly 3 months after the initial cases of the disease:
Forty Years of Marburg Virus
“In early August 1967, patients with unusual symptoms indicating an infectious disease were admitted to the university hospitals in Marburg and Frankfurt. The first patients were treated in their homes for up to 10 days, even though the illness was described as beginning suddenly with extreme malaise, myalgia, headache, and a rapid increase in temperature to as high as 39°C or more. Although the clinical symptoms were not very alarming during the first 3–4 days, additional symptoms and signs appeared at the end of the first week. Gastrointestinal symptoms, such as nausea, vomiting, and diarrhea, indicated to health care practitioners that the diagnosis might be dysentery or typhoid fever. The patients were therefore admitted to a hospital. At admission, most patients were observed to have conjunctivitis, exanthema, and enanthema, but shigellae or salmonellae were not found. During the second week after onset of disease, patient temperatures fell to 38°C, and petechiae and more-severe signs of hemorrhagic diathesis were recorded for ∼25% of patients. As indicated by transaminase levels, liver destruction reached its maximum at days 7 and 8 after onset of disease. Leukopenia with the appearance of immature polymorphonuclear leukocytes and thrombocytopenia (<10,000 cells/mm3) were detected. Patients were bleeding from all body orifices and from needle punctures. When the outcome was fatal, death occurred during the second week after onset of disease, at day 9 on average (range, day 7–16). In some cases, patients died from severe hemorrhagic shock on the day after hospital admission. Severe hemorrhagic signs, as seen in ∼25% of patients, were a signum mali ominis. All patients who died had hemorrhaging. Of 7 patients with manifest hemorrhages, 5 succumbed to the disease. Orchitis, a typical late-stage symptom, appeared in the third week after onset of disease or even at relapse during the fifth week. Mental confusion and paraesthesias were indicative of cerebral involvement. Relapses with hepatitis, orchitis, and uveitis with virus persisting in semen and in the anterior eye chamber were typical during the convalescent phase of both Marburg virus (MARV) and Ebola virus (EBOV) infections. In 1 case, a patient transmitted infection to his wife 120 days after onset of his disease, most probably by sexual intercourse. Virus was detectable in seminal fluid.
The incubation time of MARV disease could only be estimated retrospectively, after the source of infection and the date of exposure were known. Incubation ranged from 5 to 9 days, with an average of 8 days. The ratio of primary to secondary infections was 21:3 in Marburg, 4:2 in Frankfurt, and 1:1 in Belgrade. Three cases of secondary infection resulted from inadvertent needle-stick inoculations; in 1 case, a pathology technician cut himself on the forearm with a knife during a postmortem examination. Airborne transmission between humans did not occur, as indicated, for example, by the instance of a young man who slept in the same bed with his brother only a couple of days before he died; the brother did not develop disease and was seronegative for MARV 6 months later. One of the patients had been severely ill at the time of the outbreak but, for unknown reasons, was not hospitalized. He recovered and, 15 years later, maintained that he had had MARV disease. At that time, he underwent serological testing and was found to be seropositive for MARV antibody by IFA and ELISA. He had been exposed to monkey kidney cell cultures, which were used for the production of poliomyelitis vaccine. At 6 months after the outbreak, blood specimens were obtained from 120 persons who had been in close contact with patients or with infectious material but who had not developed disease. The specimens were tested for MARV antibody by complement fixation test, IFA, and ELISA and were found to be seronegative. Therefore, there was no indication of clinically inapparent infection.”
“By mid September, it had become evident that the agent exhibited a low contagiousness. Only a few cases of secondary infection and no cases of tertiary infection had occurred, and no new cases had occurred during the previous 2 weeks. Therefore, Rudolf Siegert (figure 1) resumed experiments with guinea pigs, together with a Chinese colleague, Hsin Lu Shu. They found that the agent could be passed among guinea pigs and exhibited pathogenicity that increased from passage to passage. At the third passage, the animals fell ill with fever, hepatitis, and hemorrhagic disease that closely resembled human disease, and they died within 10 days after inoculation, with a marked drop in temperature. However, all efforts to determine the etiological agent by light or electron microscopy failed. Opportunistic bacterial infections were a major problem.
At this time, specimens of human and guinea pig convalescent serum were available, and some of the serum specimens were tagged with fluorescein for direct IFA. Three weeks later, W.S. (figure 1) detected intracytoplasmic inclusions in the tissues of infected guinea pigs, by IFA. Animals that had infected cells in the liver and spleen were selected for further studies using electronmicroscopy. Blood specimens from these animals were inactivated with formalin and sent to Dietrich Peters at the Bernhard Nocht Institute in Hamburg. Formalinized plasma was spun directly onto electron microscope (EM) grids, by means of a new technique developed by Gerhard Müller, and negative staining was done. By these methods, MARV was identified on 20 November, < 3 months after the outbreak had begun (figure 2).”
https://academic.oup.com/jid/article/196/Supplement_2/S131/858753
It needs to be noted that, according to Slenczka’s account of the events, no “virus” was ever properly purified and isolated at any point during the investigation into the potential cause of disease afflicting the laboratory workers in 1967. In fact, the initial evidence for the existence of the Marburg “virus” essentially boiled down to experimentally making Guinea pigs sick through serial passaging of unnatural injections of blood/tissues into their stomachs, examining their spleens and livers using non-specific antibodies to find non-specific inclusions, and then taking electron microscopy images of the sickened animals blood and claiming random particles seen in the unpurified and contaminated samples are the “virus” in question. Eventually, after many unsuccessful attempts of trial and error failures, it was claimed that the “virus” could be propagated in cell culture (without CPE) using the Guinea pig (not human) materials.
For a better understanding of the fraudulent methods used to propagandize the public on a new deadly “virus,” let’s break down the main three focus areas (animal experiments, EM imaging, and cell culture) even further and see what the evidence shows.
1. Animal Experimentation

“Experimental infection apparently results in 100% fatality. If this situation occurs in nature, obviously there could not be any serologic positives. However, if the experimental route of inoculation differs from that occurring in nature, it is possible that 100% fatality will not develop.”
https://link.springer.com/chapter/10.1007/978-3-662-01593-3_22
The first piece of evidence used for the existence of a new “virus” was the creation of “similar” symptoms in Guinea pigs by continually injecting them with serially passaged diseased fluids/tissues. What these injections actually contained is difficult to determine as the original study is in German and the translation is not clear. The study, lead by Rudolf Siegert, mentioned doing successive passages with whole blood, plasma or organ material yet what the exact methods were beyond that remain obscure due to a faulty translation.
Fortunately Rudolf Siegert collected much of the Marburg research into a book in 1971. Oddly, he did not include his original paper On the etiology of an unknown human infection originating from monkeys yet he did provide a study explaining the procedures used for passaging the “virus” in Guinea pigs which furnished some insight into the kind of experiments that were ultimately carried out. What we can see in the highlights from the included paper below is that the clotted blood was haemolyzed with sterile distilled water and the organs triturated using a cold mortar. A phosphate buffer diluent containing 10 p. 100 normal rabbit serum was added to the blood mixture which was used to inject mice intracerebrally (in the brain) and intraperitoneally (in the stomach) as well as Guinea pigs intraperitoneally. The researchers admitted that all “isolation” attempts were negative except for in Guinea pigs as, after injecting the Guinea pigs in the stomach with blood samples, organ suspensions, and Cercopithecus organ pools, the animals developed a febrile (fever) reaction 4 to 6 days after inoculation. Clinical symptoms in the animals included loss of appetite and weight, “bloated face,” and enlargement of the testes. The researchers concluded that from the human and monkey material, an organism was “isolated” and transmitted through four to six passages in Guinea pigs even though no “virus” was ever purified, isolated, and visualized:
Passage of Marburg Virus in Guinea Pigs
“Clotted blood was haemolyzed with sterile distilled water and the organs triturated using a cold mortar and phosphate buffer diluent containing 10 p. 100 normal rabbit serum added to give a final concentration of about 20 percent by volume.”
“Suckling mice were inoculated intracerebrally (ic) and intraperitoneally (ip) with 0.02 ml.
Guinea pigs (200-300 g) were inoculated ip with 4 ml. For further passaging, whole blood harvested by cardiac puncture was injected ip.”
Results
All isolations attempts have been negative except in guinea pig.
Guinea pig Passages
Guinea pigs injected by ip route with blood samples of patient H. F. (HF 1 and HF 2) organ suspensions of patient P. S. and Cercopithecus organ pools M 10 and M 14 consistently developed a febrile reaction 4 to 6 days after inoculation.
The febrile stage lasted 3 to 7 days.
Whole blood taken during this febrile stage has been successfully passaged ip in guinea pigs through 3 to 6 passages (Figs. 1 to 5). The incubation period was shortened to 2-3 days and some guinea pigs died from 7 to 17 days after inoculation. Clinical symptoms in the animals were: loss of appetite and weight, “bloated face” and enlargement of the testes. At autopsy, we found splenomegaly and lung consolidation.
Fever reactions in guinea pigs were produced using early blood samples from the preceding passage. In one instance (Fig. 4, passage 4), fever reaction followed inoculation of blood taken at the 11th day. This fact confirms observation that infection seems to produce a long lasting viraemia.”
Conclusions
“The results reported above show that from human and monkey material, an organism has been isolated and transmitted through four to six passages in guinea pigs.”
DOI: 10.1007/978-3-662-01593-3_16
As can be seen from the above study, the researchers are conflating the experimental creation of disease in Guinea pigs through serial passaging and unnatural routes of infection with the “isolation” of a “virus.” At no point was a “virus” ever purified and isolated from the fluids of a sick human, a monkey, nor a Guinea pig. Beyond the non-specific fever, weight loss, and loss of appetite (occuring after injections of toxic unpurified goo into the stomach), none of the symptoms experienced by the Guinea pigs (bloated face, enlarged testes) related to the human condition whatsoever. In fact, Rudolf Siegert and Werner Slenczka later admitted in their paper Laboratory Diagnosis and Pathogenesis, that regarding the pathogenesis of the disease in man, “apparently the virulence of
the Marburg virus differs in monkey, man, and guinea pig.” Yet it was based on these experimental results that it was determined a new pathogenic “virus” was hiding in the fluids of the sickened Guinea pigs which were then used for electron microscopy imaging in order to try and find the new “virus.”
2. Electron Microscopy Images

The second possibility of making a rapid diagnosis lies in the direct demonstration of the virus with the electron microscope. This may succeed if the agent is directly centrifuged from serum or plasma on a carrier, according to Peters and Muller [7]. The characteristic morphology leaves no doubt as to the diagnosis. However, we have no experience enabling us to answer the question concerning
https://link.springer.com/chapter/10.1007/978-3-662-01593-3_22
the probability that the agent may be overlooked with this method. It is for this reason that attempts to isolate the virus in guinea pigs and in various cell culture systems should follow in any case.
While the researchers failed in their initial attempts to identify the “virus” by electron microscopy after sickening the Guinea pigs, they eventually determined through direct and indirect antibody staining results that they could find the “virus” in the livers and spleens of these animals. While Rudolf Siegert’s study did not offer much insight into how they determined that the particles observed were the actual “virus” they were looking for, he did offer some interesting comments about their morphology which fortunately were not lost in translation:
On the etiology of an unknown human infection originating from monkeys
“The results described show that “Marburg Virus” is not identical, but it is morphologically closely related to the virus vesicular stomatitis (1, 2, 6, 9, 11, 12), the Coval (1, 3) Egtved- (13) and finally the rabies virus (8, 10). A fundamental difference from these viruses seems to have the particular tendency to be growth in length.”
DOI: 10.1055/s-0028-1106144
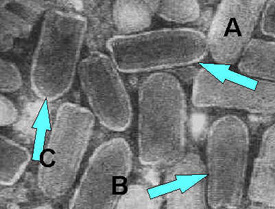
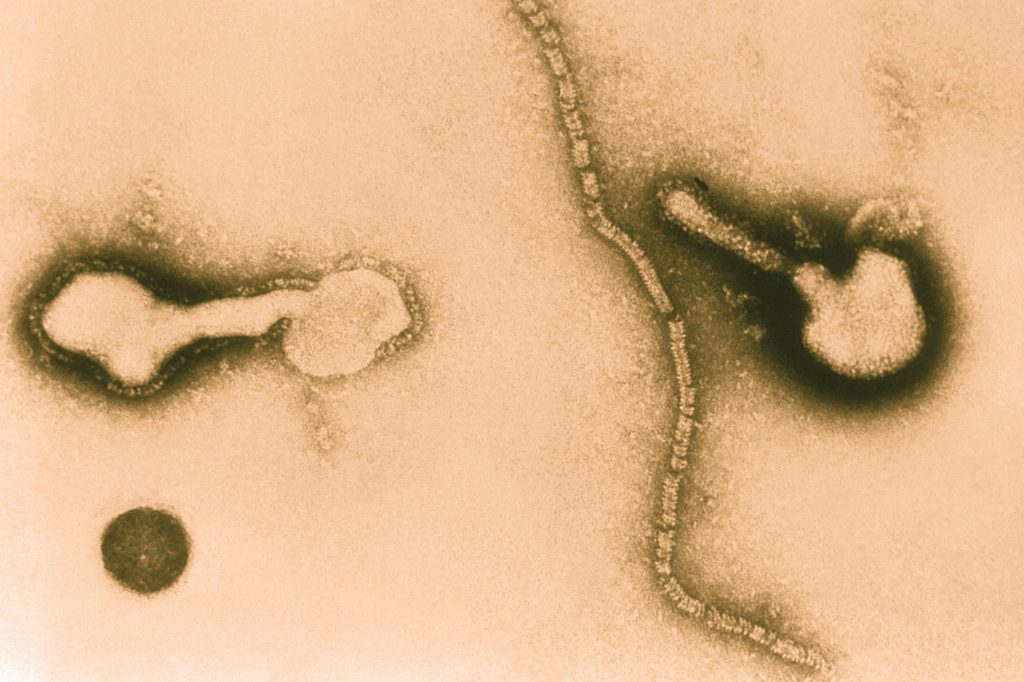
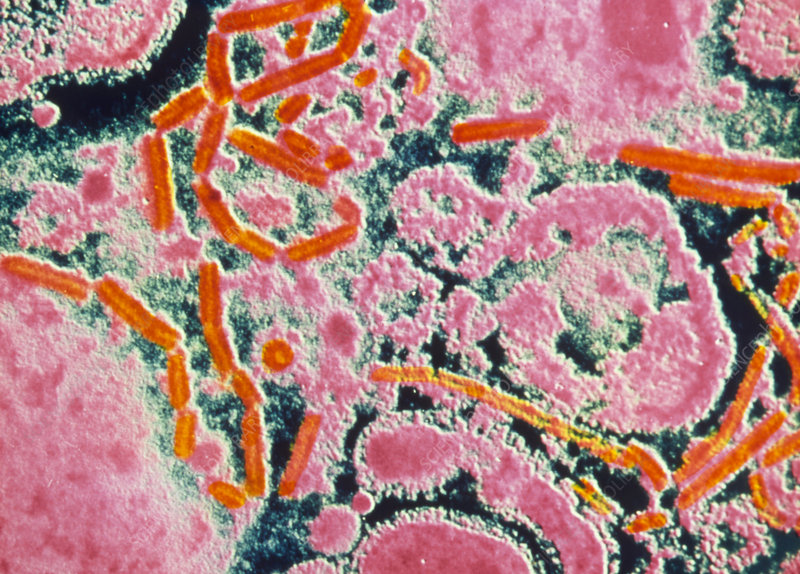
According to Seigert, the particles he observed looked morphologically like the vesicular stomatitis, coval, egtved, and rabies “viruses.” The main difference was in the length of the particles. However, does the length of the particles really distinguish these “viruses” from each other all that much? Could these all be random pieces from the same long strands broken apart or even created from the procedures used to capture the images? Presented below are the images of the Marburg “virus” supplied by Seigert which show some longer particles mixed with other smaller particles which resemble the bullet shape of the aforementioned “viruses” listed in his paper. The third image included is one provided by Slenczka said to be from the original “isolate” in 1967 while the colorized pictures are images taken from recent 2022 articles on the Marburg “virus” cases in Ghana:



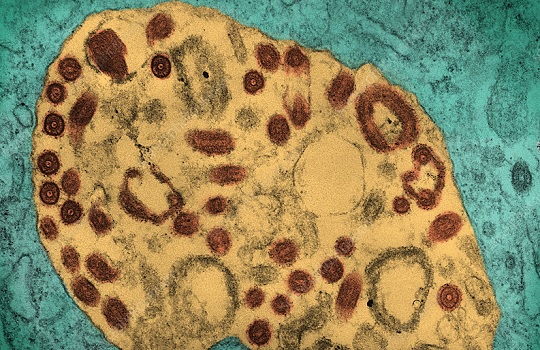

As can be seen, the Marburg “virus” comes in different shapes and sizes, from long filament particles to smaller bullet-like particles to even those resembling “corona-like” structures. It seems that the image of the “virus” heavily depends upon the way the picture is taken/cropped as well as how the particles are stained and colorized. Below are images of the “viruses” said by Seigert to be morphologically similar to the Marburg “virus:”
Vesicular Stomatitis
In these images, we can see the similar bullet-like shape in the vesicular stomatitis “virus” as seen in the particles claimed to be the rabies “virus.” Interestingly, the particles appear to vary in size from the smaller bullets to the much more elongated forms resembling the Marburg “virus.” This “unwinding” was described in the third image as most likely a result of the negative staining procedures done to visualize the “virus” particles.



Viral Haemorrhagic Septicemia Virus (VHSV)
The VHSV is a fish “virus” that also supposedly shares the exact same shape as the rabies “virus” and is morphologically similar to the Marburg “virus.” As can be seen, the shapes of the particles once again range from small bullet-like entities to longer filaments, perhaps caused once again by the negative staining procedures.


Rabies
Even the rabies “virus,” said to be the bullet-like particles seen in the TEM images, show various shapes and sizes depending on the staining and colorization. Some appear to be long Marburg-like filament forms that happen to be present in a U-shape upon imaging. Interestingly enough, up to the early 1980’s, the Marburg “virus” was classified as a rhabdovirus due to the similarities between the morphology of the “viruses.” It was even originally given the moniker Rhabdovirus simiae.


While it is easy to see the similarities between the Marburg “virus” and the other “viruses” Seigert highlighted in his study, he failed to mention that we can find similar looking filament particles associated with many other “viruses” as well:
Mumps



Measles



Parainfluenza


It can be seen that the images of these particles claimed by Seigert to be of different “viruses” definitely share similar morphology (i.e. form and structure). It is clear that the staining and colorization of the particles as well as how they are zoomed in and presented definitely influences how they appear in the images. It is even stated in one study that the negative staining procedures have an impact on how the particles form. It is evident, when including images of filament forms of other “viruses,” that this is yet another case where the same particles (seen in various stages of formation/degradation) are being cropped from an unpurified sea of different shapes and structures and focused on as the representative culprit in numerous diseases.
As the electron microscopy images play such a pivotal role in the proof supplied for the Marburg “virus,” it is important to gain some greater insight into the electron microscopy process used by Werner Slenczka and Co. in order to identify the Marburg “virus.” For this we can now turn our attention to a 2017 article he wrote describing how his “filovirus” research began. In this account, we find out that the blood samples taken from the Guinea pigs were mixed with glutaraldehyde and formaldehyde before imaging. Slenczka admitted that searching for an unknown pathogenic agent in EM can be fatiguing and frustrating as he explained that many contaminants can be found within the sample. This was the case with the Marburg “virus” as numerous microbial contaminants were present in the sample (thus it was unpurified and not isolated) which made the interpretation of the data difficult. As stated before, the spleens and livers of the Guinea pigs were used for EM imaging utilizing direct and indirect antibody fluorescence, and the samples were air-dried and fixed with ice-cold acetone. Since they did not know if the unknown agent would be killed by acetone, Slenczka claimed that they handled the slides with extreme caution. It then took them 3 weeks of hard work to get the initial results. Slenczka stated that what he saw in his slides resembled the Negri bodies said to be specific to the rabies “virus” yet somehow this finding told him that this effect was the cause of a new “virus.” He used his initial findings to mark any Guinea pig sample with these inclusions as ones with the “virus” in need of further analysis by EM.
The blood samples which were selected for further analysis were once again subjected to glutaraldehyde and formaldehyde and studied. Dr. D. Peters, along with his technician, spent more than a day looking through the samples with no results. On the second day, Dr. Peters left the search for a lunch break and handed the reigns to Dr. G. Müller. Once Dr. Peters arrived back from his lunch break, he was informed by Dr. Müller that the “virus” had been found (in less than an hour) as they had observed unknown particles of a different morphology and structure to any that had been seen before. Obviously, this is not the case as these same particles have been observed with various “viruses” as detailed previously. Ultimately, the entire “isolation” process did not involve the purification and isolation of any “virus” directly from human fluids and instead relied entirely on assumptions based on indirect evidence obtained from animal, antigen, and EM studies using unpurified and non-isolated material from Guinea pigs rather than humans.
Interestingly, as the laboratory researchers who were initially “infected” with the “virus” were conducting polio vaccine research using monkey kidney cell cultures, it was assumed that the “virus” came from the imported monkeys. However, according to Slenczka, none of the monkeys at any of the laboratories ever showed any signs of disease at any location. He also stated that the exact lethality data of the incriminated monkeys was never communicated. Thus, it was left up to mere assumptions that some persistently infected monkeys from “Monkey island” which were caged for research may have been the source for importing Marburg “virus” to Europe. According to Slenczka, it was known that a large number of monkeys from the same source in Uganda were transported to Sweden, Japan, Czechoslovakia, Italy, Switzerland, and England at the same time for the purpose of preparing cell cultures. However, no outbreaks were reported at any of these locations. Thus, Slenczka was forced to admit that his hypothesis, just like his “virus,” was solely based on assumptions:
Filovirus Research: How it Began
“These experiments were a step in the right direction, but the agent remained unidentified. To facilitate identification, blood from infected animals, taken at the climax of the disease, was mixed with glutaraldehyde and formaldehyde to inactivate and preserve the unknown agent and was sent to the electron microscopy (EM) laboratories at the University of Marburg and the Bernhard Nocht Institute for Tropical Medicine in Hamburg, Germany for analysis: Dr. D. Peters, head of the
Virology Department at the Bernhard Nocht Institute, was a renowned virological electron microscopist and highly experienced in analyzing viral structures.
Of course, EM-based search for an unknown pathogen in biological materials can be extremely fatiguing and––in case of a negative result––very frustrating.
In the case of the guinea pig material, an additional obstacle became evident soon. A serious complication, often encountered in the search for unknown pathogens, is contamination by organisms unrelated to the disease. These “pick-up” contaminants may interfere with the etiological agent or may even cause disease themselves. Contamination may occur as a result of a preexisting infection. During passage to new animals, contaminants might be transferred with a higher efficiency than the unknown etiological agent. The risk of cultivating a contaminating agent may be reduced by using animals from an SPF (specific pathogen free) breed. In 1967, SPF guinea pigs could not be afforded in Marburg. Instead, the animals were purchased from local breeding stations which did not control for infections. Therefore, in the experiments carried out by Drs. Siegert and Shu, it happened that microbial contaminations, including pseudomonads, pasteurellae, and in some cases paramyxoviruses were present in the guinea pigs. Although it was quite clear that these well-known organisms were not the etiological pathogen, the presence of these contaminants complicated data interpretation.”
“Organs from infected and noninfected guinea pigs, especially livers and spleens, were used to make imprint preparations on microscopic slides, which were then air-dried and fixed with ice-cold acetone. Since we did not know if the unknown agent would be killed by acetone, we handled these slides with extreme caution. It took 3 weeks of hard work before we had the first results. I found brilliantly fluorescent cytoplasmic inclusions in liver cells from an infected guinea pig. Since all the controls were negative, I was sure I had found antigenic structures of the unknown pathogen (Fig. 4). At this time, it was not yet possible to tell whether these inclusions, which resembled the Negri bodies found in rabies virus-infected cells (Goldwasser et al. 1959), were indicative of a viral or bacterial infection. However, it was clear that I had detected something that nobody had seen before; structures of an unknown agent causing a deadly disease (Slenczka et al. 1968).
Using this assay, it was now possible to identify those animals which were infected with this agent to select material for EM investigations. Once again, guinea pig blood treated with glutaraldehyde and formaldehyde was sent to the Bernhard Nocht Institute in Hamburg for EM analysis. Dr. D. Peters, together with a technician, analyzed negative stained material for more than a day but did not observe anything reminiscent of a viral structure. On the second day of his search, Dr. Peters left the laboratory for a lunch break and handed the specimen to his coworker, Dr. G. Müller, asking him to continue the search. In less than an hour, Dr. Müller had succeeded in finding viral particles that, due to their sizes and unique morphologies, were identified as the products of an unknown virus (Fig. 5). When Dr. Peters returned from his lunch break, Müller showed him the new virus. It is not clear why Dr. Peters had not found the viral particles when he examined the samples. The most probable explanation seems to be that the particles had spontaneously sedimented to the bottom of the tube and Dr. Peters took material from the top only.”
“The researchers who deserve credit for isolating and identifying Marburg virus are Walter Mannheim, University of Marburg for successful transmission to guinea pigs, Werner Slenczka, University of Marburg for detecting and identifying the Marburg virus antigen by immunofluorescence analysis, and Gerhard Müller, Bernhard Nocht Institute for identifying the virus by EM. Walter Mannheim, a bacteriologist, was uninterested in co-authoring publications despite his involvement in the virus isolation.”
“The most intriguing question regarding these monkeys is their state of health. Where and at what time did they acquire the virus? Why did they not show signs of disease at any location; not when they were in Entebbe, not upon their arrival in London, Frankfurt, Marburg, or Belgrade, and not when they were finally euthanized? The lethality of imported NHPs was about 5% at that time. An increase in lethality of imported NHPs should certainly have raised suspicion. Exact lethality data of the incriminated monkeys were never communicated. There can be no doubt that the animals were inspected carefully before they were used.”
“Assuming that some persistently infected monkeys from “Monkey island” could have been the source for importing Marburg virus to Europe might help to explain some peculiarities of this outbreak. It is known that a large number of monkeys from the same source in Uganda were transported to Sweden, Japan, Czechoslovakia, Italy, Switzerland, and England at the same time and for the same purpose: to prepare cell cultures. But no outbreaks were reported at any of these locations. It is possible that when the shipments to Germany and to Yugoslavia were assembled, there were not enough monkeys left at the collecting station and therefore, that animals from “Monkey island” were used to supplement the shipment. Among the animals captured from “Monkey island” were possibly some which had survived an infection with Marburg virus but appeared to be healthy. This might explain why Marburg virus was exclusively transported with shipments to locations in Germany and in Yugoslavia.
Admittedly, the above-formulated hypothesis is based on assumptions. But it offers an intriguing explanation addressing many of the open questions regarding this outbreak that, until now, have remained unanswered.”
https://pubmed.ncbi.nlm.nih.gov/28766193/
3. Cell Culture

In cell cultures cytopathic alterations are absent. However, as early as the
https://link.springer.com/chapter/10.1007/978-3-662-01593-3_22
third day cytoplasmic antigen inclusions may be recognized, which increase considerably in number and size until the 7th day.
Beyond the issues related to the interpretation of contaminated and unpurified EM images and the lack of disease in the monkeys assumed to have been carriers of the “virus,” early attempts to propagate the “virus” in cell cultures failed miserably. Many different cell lines were used and conflicting results were often obtained. Many times, the researchers claimed that the “virus” successfully replicated in the cells even though the required cytopathogenic effect (CPE) was never observed. This is the effect which virologists use to claim that the structural changes observed in a host cell during culturing are the result from “viral” infection and replication. As one source stated, the CPE is a way of “seeing” and indirectly measuring a “viral” infection by looking at the damage a “virus” causes to a cell. This damage is a measurement that is widely used in virology labs all over the world in order to determine indirectly the presence of a “virus.” Without observing such an effect, the culture should theoretically show that no “virus” is present in the sample. However, as this effect is not always observed, virologists found a way around the lack of being able to produce this effect in all cultures by claiming that some “viruses” do not produce CPE at all while others only do so in certain cell lines. They state that even without the observance of CPE, the cultures are still successful despite the lack of any structural changes denoting the highjacking of the cell by the “virus” and the subsequent replication process.
The below highlights are from a 1971 paper which summarized the attempts to cultivate the Marburg “virus” and explained the confusing and contradictory results. The authors concluded that while the “virus” could be propagated in culture, the general rule was that no gross cytopathic changes could be observed:
Cultivation of the Marburg Virus (Rhabdovirus simiae) in Cell Cultures
“At the time when the causative agent of Marburg haemorrhagic fever was still unknown, attempts were made to isolate the agent from patients. For isolation purposes laboratory animals and many cell systems were employed but all initial trials in cell cultures were unsuccessful (SIEGERT et aI., 1967; MAY and KNOTHE,1968; SIEGERT et aI., 1968). Later when the virus was isolated in guinea pigs (SIEGERT et aI., 1967; SMITH et aI., 1967; KUNZ et aI., 1968; MAY and KNOTHE, 1968; KISSLING et aI., 1968), many investigators tried to propagate Marburg virus in various cell cultures. Presently, much data are available which will be summarized in this report.”
In primary cells of Cercopithecus kidney, the species with which the agent was imported to Germany, SIEGERT et aI. (1968) found that the virus replicated without cytopathic effect (CPE). They also demonstrated the virus specific antigen by means of the immunofluorescent method. On the contrary HAAS et aI. (1968) observed gross CPE in primary Cercopithecus kidney cells. These cells were only less sensitive to the virus than subcutaneously infected Cercopithecus monkeys.
In primary Rhesus monkey kidney cells, the virus replicated but without CPE (HOFMANN and KUNZ, 1968). Primary cells of human origin also propagated the virus. MAY and KNOTHE (1968) could not observe CPE in human leucocytes but reported slight CPE in primary human amnion cells (MAY et aI., 1968).
We could demonstrate replication of the virus in primary guinea pig embryo fibroblasts but no CPE was seen (HOFMANN and KUNZ, 1968).
In chick embryo cells, we found a very slight virus replication (HOFMANN and KUNZ, 1968), while other investigators did not observe propagation at all (SMITH
et aI., 1967; MAY and KNOTHE, 1968).”
“Established cell lines were also investigated for propagation of Marburg virus. At first cells derived from monkeys were tested. Although we found that permanent Cercopithecus kidney cells (strain GMK-AHl) produced high titers of virus-1 ml of culture fluid contained 10^6 infective doses for guinea pigs-we could not demonstrate any CPE. KISSLING et aI. (1968) were more successful; they observed CPE in their cultures in the second day p.i., which was in total about the 4th-5th day.
In the VERO cell line, the virus also propagated. No CPE was observed by SIEGERT et aI. (1968) and only slight CPE by KISSLING et aI. (1968).
From cells of Rhesus monkey origin, heart cells (strain CMH) allowed only slight virus growth (HOFMANN and KUNZ, 1968), while in kidney cells (strain LLC-MK2) no virus replication was demonstrable (SMITH et aI., 1967).
In the studies of SMITH et aI. (1967) the Marburg virus propagated in L cells (mouse embryo cells) without CPE; we could not demonstrate any virus growth in those cells.
Heart cells derived from guinea pigs also allowed virus replication without CPE (KISSLING et aI., 1968).
The first reports of Marburg virus-induced CPE in cell cultures were by ZLOTNIK et aI. (1968). They had found that the virus was adaptable to BHK21 cells. In the first passage typical inclusion bodies similar to those found in guinea pig liver, were seen in infected cells after 13 days and CPE appeared about the 23rd day. After a few passages, inclusion bodies as well as CPE appeared earlier. In our laboratory BHK21 cultures showed only slight changes which appeared very late (HOFMANN and KUNZ, 1968). KISSLING et aI. (1968) tested two strains of BHK21 . One, the WI 2 strain, behaved as the strain in our laboratory, but the other was highly susceptible. Cytopathic effect was observed about the 2nd-5th day after infection.
In contrast to 3 other teams of investigators (SIEGERT et aI., 1968; SMITH et aI., 1967; MAY and KNOTHE, 1968), we could propagate Marburg virus quite well in our HeLa strain. One ml of culture fluid contained 104 infective particles for guinea pigs, however we found no CPE (HOFMANN and KUNZ, 1968).
Other strains deriving from human sources were also tested for Marburg virus induced CPE. KISSLING et aI. (1968) propagated the virus in foreskin fibroblastsIn the first passage of virus CPE was demonstrable but could not be reproduced in serial passages. In U cells, a stable cell line of human amnion, the agent also replicated but without CPE (HOFMANN and KUNZ, unpublished).
In our laboratory we had previously tested many cell systems, but we were unable to detect a cell line in which Marburg virus propagates with CPE. Finally we came across the ELF (embryonal human lung fibroblasts) cell strain, in which CPE appears about the 3rd day and reaches its maximum about the 5th day after infection. Cytopathic effect begins in focal areas and consists of spindling and later on of clumping of cells. Finally the foci become confluent (see Figs. 1-3). It must be mentioned that, although changes are severe, they are never complete and eventually healthy cells may grow in and repair the lesions.”
“Summarizing the sometimes conflicting results obtained by the various investigators, it can be stated that cells deriving from mammals such as monkey, guinea pig, and hamster and human cells are susceptible to the virus. Often high titers were produced by the cells although as a rule no gross cytopathic changes could be observed.”
https://link.springer.com/chapter/10.1007/978-3-662-01593-3_15

In Summary:
- Marburg “virus” disease (MVD) is said to be a rare but severe hemorrhagic fever which affects both people and non-human primates
- It is one of seven belonging to the Filoviridae group, with the other six species of Ebola “virus” the only other known members of the “filovirus” family
- Marburg “virus” was first recognized in 1967, when outbreaks of hemorrhagic fever occurred simultaneously in laboratories in Marburg and Frankfurt, Germany and in Belgrade, Yugoslavia (now Serbia)
- The first people “infected” had been exposed to Ugandan imported African green monkeys or their tissues while conducting research
- Clinical diagnosis of Marburg “virus” disease (MVD) can be difficult as many of the signs and symptoms of MVD are similar to other infectious diseases (such as malaria, typhoid fever, or dengue) or “viral” hemorrhagic fevers that may be endemic in the area (such as Lassa fever or Ebola)
- The first patients were treated in their homes for up to 10 days, even though the illness was described as beginning suddenly with extreme malaise, myalgia, headache, and a rapid increase in temperature to as high as 39°C or more
- Although the clinical symptoms were not very alarming during the first 3–4 days, additional symptoms and signs appeared at the end of the first week
- Gastrointestinal symptoms, such as nausea, vomiting, and diarrhea, indicated to health care practitioners that the diagnosis might be dysentery or typhoid fever
- In some cases, patients died from severe hemorrhagic shock on the day after hospital admission
- Note that there is zero information on what treatments the patients underwent before and after admission to the hospital which could have worsened their clinical symptoms
- Airborne transmission between humans did not occur, as indicated, for example, by the instance of a young man who slept in the same bed with his brother only a couple of days before he died; the brother did not develop disease and was seronegative for MARV 6 months later
- One of the patients had been severely ill at the time of the outbreak but, for unknown reasons, was not hospitalized and recovered and, 15 years later, maintained that he had had MARV disease (full recovery from severe illness without hospital admission/treatment… 🤔)
- By mid September, it had become evident that the agent exhibited a low contagiousness
- Only a few cases of secondary infection and no cases of tertiary infection had occurred, and no new cases had occurred during the previous 2 weeks
- Rudolf Siegert performed experiments with Guinea pigs and found that the agent could be passed among Guinea pigs and exhibited pathogenicity that increased from passage to passage (i.e. the more they injected Guinea pigs with cultured diseased goo and tissues, the more they became sick)
- However, all efforts to determine the etiological agent by light or electron microscopy failed and opportunistic bacterial infections were a major problem
- In other words, they claimed there was a “virus” inside the toxic goo serially passaged and injected into Guinea pigs but they could not find it
- After this failure, specimens of human and Guinea pig convalescent serum were available, and some of the serum specimens were tagged with fluorescein for direct IFA
- Three weeks later, W.S. detected intracytoplasmic inclusions in the tissues of infected guinea pigs, by IFA
- Formalinized plasma was spun directly onto electron microscope (EM) grids, by means of a new technique developed by Gerhard Müller, and negative staining was done
- By these methods, the Marburg “virus” was identified on November 20, 1967, almost 3 months after the outbreak had begun
- For the Guinea pig experiments, clotted blood was haemolyzed with sterile distilled water and the organs triturated using a cold mortar and phosphate buffer diluent containing 10 p. 100 normal rabbit serum added to give a final concentration of about 20 percent by volume
- Suckling mice were inoculated intracerebrally (IC) and intraperitoneally (IP) with 0.02 ml while Guinea pigs (200-300 g) were inoculated IP with 4 ml
- For further passaging, whole blood harvested by cardiac puncture was injected IP
- All isolations attempts were negative except in Guinea pigs
- Guinea pigs injected by IP route with blood samples of patient H. F. (HF 1 and HF 2) organ suspensions of patient P. S. and Cercopithecus organ pools M 10 and M 14 consistently developed a febrile reaction (i.e. fever) 4 to 6 days after inoculation
- Whole blood taken during this febrile stage had been successfully passaged IP in Guinea pigs through 3 to 6 passages
- The incubation period was shortened to 2-3 days and some Guinea pigs died from 7 to 17 days after inoculation
- Clinical symptoms in the animals were:
- Loss of appetite and weight
- “Bloated face”
- Enlargement of the testes
- The researchers felt that the results reported showed that from human and monkey material, an organism had been “isolated” and transmitted through four to six passages in Guinea pigs
- In other words, injecting diseased tissues and fluids successively into Guinea pigs and causing symptoms equalled “isolating a virus”
- According to the electron microscopy imaging search for the “virus,” Rudolf Siegert described the particles seen as morphologically closely related to the vesicular stomatitis “virus,” the Coval, Egtved, and the rabies “virus”
- A fundamental difference from these “viruses” seemed to have the particular tendency to grow in length
- In order to identify the “virus” particles in EM, blood from infected animals, taken at the climax of the disease, was mixed with glutaraldehyde and formaldehyde to inactivate and preserve the unknown agent
- Werner Slenczka admitted that EM-based search for an unknown pathogen in biological materials can be extremely fatiguing (which would not be the case in a purified/isolated preparation)
- A serious complication, often encountered in the search for unknown pathogens, is contamination by organisms unrelated to the disease
- These “pick-up” contaminants may interfere with the etiological agent or may even cause disease themselves
- During passage to new animals, contaminants might be transferred with a higher efficiency than the unknown etiological agent
- In 1967, special pathogen-free guinea pigs could not be afforded in Marburg so the animals were purchased from local breeding stations which did not control for infections
- Therefore, in the experiments carried out by Drs. Siegert and Shu, it happened that microbial contaminations, including pseudomonads, pasteurellae, and in some cases “paramyxoviruses” were present in the guinea pigs
- The presence of these contaminants complicated data interpretation
- Samples were air-dried and fixed with ice-cold acetone yet, as they did not know if the unknown agent would be killed by acetone, they handled these slides with extreme caution
- It took 3 weeks of hard work before they had the first results
- Slenczka found inclusions within the samples which resembled the Negri bodies found in rabies “virus-infected” cells
- Somehow, finding the same inclusions as seen in rabies led Slenczka to believe that this was the result of a new “virus”
- Dr. D. Peters, together with a technician, analyzed negative stained material for more than a day but did not observe anything reminiscent of a “viral” structure
- On the second day of his search, Dr. Peters left the laboratory for a lunch break and handed the specimen to his coworker, Dr. G. Müller, asking him to continue the search and in less than an hour, Dr. Müller had succeeded in finding “viral” particles that, due to their sizes and unique morphologies, were identified as the products of an unknown “virus”
- Remember that it was admitted that the Marburg “virus” resembled many other “viruses,” including rabies, morphologically
- It is not clear why Dr. Peters had not found the “viral” particles when he examined the samples
- According to Slenczka, the researchers who deserve credit for “isolating” and identifying Marburg “virus” are:
- Walter Mannheim, University of Marburg for successful transmission to guinea pigs (he was uninterested in co-authoring publications despite his involvement in the “virus” isolation)
- Werner Slenczka, University of Marburg for detecting and identifying the Marburg “virus” antigen by immunofluorescence analysis
- Gerhard Müller, Bernhard Nocht Institute for identifying the “virus” by EM
- Note that the entire “isolation” process did not involve the purification and isolation of any “virus” directly from human fluids and instead relied entirely on assumptions based on indirect evidence obtained from animal, antigen, and EM studies using unpurified and non-isolated material from Guinea pigs
- As the laboratory workers who were sickened were working on polio research using monkey kidney cell cultures, it was assumed that they had become infected from the imported monkeys
- However, none of the monkeys showed signs of disease at any location
- Exact lethality data of the incriminated monkeys was never communicated
- Slenczka assumed that some persistently infected monkeys from “Monkey island” could have been the source for importing Marburg “virus” to Europe
- It was known that a large number of monkeys from the same source in Uganda were transported to Sweden, Japan, Czechoslovakia, Italy, Switzerland, and England at the same time and for the same purpose: to prepare cell cultures
- However, no outbreaks were reported at any of these locations
- Slenczka admitted that his formulated hypothesis was based on assumptions
- As stated before, the attempts to isolate a “virus” from human patients failed
- For isolation purposes laboratory animals and many cell systems were employed but all initial trials in cell cultures were unsuccessful
- It wasn’t until when the “virus” was “isolated” in guinea pigs that further attempts to culture a “virus” were made
- Many investigators tried to propagate Marburg “virus” in various cell cultures
- In primary cells of Cercopithecus kidney, the species with which the agent was imported to Germany, Seigert et aI. (1968) found that the “virus” replicated without cytopathic effect (CPE)
- On the contrary Haas et aI. (1968) observed gross CPE in primary Cercopithecus kidney cells
- In primary Rhesus monkey kidney cells, the “virus” replicated but without CPE (Hofmann and Kunz, 1968)
- Primary cells of human origin also propagated the “virus” yet May and Knothe (1968) could not observe CPE in human leucocytes but reported slight CPE in primary human amnion cells (May et aI., 1968)
- Hofmann and Kunz could demonstrate replication of the “virus” in primary guinea pig embryo fibroblasts but no CPE was seen
- In chick embryo cells, Hofmann and Kunz found a very slight “virus” replication while other investigators did not observe propagation at all (Smith et aI., 1967; May and Knothe, 1968)
- Although Hofmann and Kunz found that permanent Cercopithecus kidney cells (strain GMK-AHl) produced high titers of “virus,” they could not demonstrate any CPE
- Kissling et aI. (1968) were more successful; they observed CPE in their cultures in the second day p.i., which was in total about the 4th-5th day
- In the VERO cell line, the “virus” also propagated while no CPE was observed by Siegert et aI. (1968) and only slight CPE by Kissling et aI. (1968)
- From cells of Rhesus monkey origin, heart cells (strain CMH) allowed only slight “virus” growth (Hofmann and Kunz, 1968), while in kidney cells (strain LLC-MK2) no “virus” replication was demonstrable (Smith et aI., 1967)
- In the studies of Smith et aI. (1967) the Marburg “virus” propagated in L cells (mouse embryo cells) without CPE yet Hofmann and Kunz could not demonstrate any “virus” growth in those cells
- Heart cells derived from guinea pigs also allowed “virus” replication without CPE (Kissling et aI., 1968)
- The first reports of Marburg “virus-induced” CPE (interesting phrase here as CPE is only supposed to be “virus-induced”) in cell cultures were by Zlotnik et aI. (1968) who found that the “virus” was adaptable to BHK21 cells
- In the first passage typical inclusion bodies similar to those found in guinea pig liver, were seen in infected cells after 13 days and CPE appeared about the 23rd day
- After a few passages, inclusion bodies as well as CPE appeared earlier (showing that the passaging caused the deterioration of the cells and the creation of the CPE, not the “virus”)
- In contrast to 3 other teams of investigators (Siegert et aI., 1968; Smitg et aI., 1967; May and Knothe, 1968), Hofmann and Kunz claimed that they could propagate Marburg “virus” quite well in HeLa strain however no CPE was observed
- Other strains deriving from human sources were also tested for Marburg “virus” induced CPE as Kissling et aI. (1968) propagated the “virus” in foreskin fibroblasts
- In the first passage of “virus” CPE was demonstrable but could not be reproduced in serial passages
- In U cells, a stable cell line of human amnion, the agent also replicated but without CPE (Hofmann and Kunz, unpublished)
- Hofmann and Kunz had previously tested many cell systems, but were unable to detect a cell line in which Marburg “virus” propagates with CPE until they came across the ELF (embryonal human lung fibroblasts) cell strain, in which CPE appears about the 3rd day and reaches its maximum about the 5th day after infection
- However, they admitted that although changes were severe, they were never complete and eventually healthy cells may grow in and repair the lesions
- Summarizing the sometimes conflicting results obtained by the various investigators, it was stated that cells deriving from mammals such as monkey, guinea pig, and hamster and human cells were susceptible to the “virus” as often high titers were produced by the cells, although as a rule no gross cytopathic changes could be observed

We are currently living in a time where novel “viruses” and old classics are seemingly breaking out in various parts of the world. Each of these outbreaks are presented by the media as potential epidemics/pandemics waiting to happen, if not now then definitely in the near future. We are being continually primed for this eventuality. What is interesting is that most of these diseases share the same non-specific symptoms including a flu-like illness and some form of rash. The diseases seem to be presenting in patients in atypical ways in non-endemic countries where the patients have no history of travel to known hotspots nor contact with any animals assumed to be carriers. As clinical diagnosis is impossible due to the overlapping symptoms, fraudulent PCR tests are being used to generate cases.
The Marburg “virus” is the latest in this “viral” merry-go-round to make an appearance. Listening to the MSM, this “highly contagious virus” has the potential to explode into the world unless it is prevented immediately, even though there are no known treatments nor vaccine which are said to be successful against it. The recent “outbreak” in Ghana infected four people while the previous “outbreak” in Guinea in 2021 infected just one. To date, there have been a grand total of 475 cases of the Marburg “virus” worldwide since its “discovery” in 1967. Is this really the “highly contagious, virulent, and lethal virus” we have been sold?
Looking into the history of the “virus” paints an entirely different picture than the one sold by the MSM. Not only was the initial outbreak among polio vaccine researchers considered not alarming from the start, the patients were treated at home for up to 10 days. Those who were eventually admitted to the hospital were the ones who ultimately succumbed as quickly as one day after admission. One patient, who was considered severely ill, never sought hospital treatment and made a full recovery. Without knowing the exact treatments given to the patients prior to and immediately after admission to the hospital, one must wonder whether the treatments caused the severity of the symptoms seen in those who ultimately succumbed to the disease.
The discovery process for the novel “virus” creates an even more convincing case that there was never any new pathogen detected. First of all, no “virus” was ever purified nor isolated directly from the fluids of a sick human nor monkey. The only evidence used to claim the existence of the Marburg “virus” comes entirely from Guinea pig experiments where unpurifued goo and tissues were injected and serially passaged in the animals. After experimentally sickening the animals, non-specific antibody testing was performed in order to find Negri-like inclusions (said to be specific to rabies but shown repeatedly not to be) in the spleens and livers of the Guinea pigs, and then blood samples were sent for electron microscopy imaging in order to find the “virus.” The hunt for the “virus” particles was long and the initial experienced researcher was unable to find anything after a day-and-a-half of searching. It wasn’t until he left for lunch that his less-experienced lab assistant was able to find the “virus” after under an hour of looking. The filament-like particles were chosen as the representative for the Marburg “virus” due to their uniqueness and length. However, as admitted by lead researcher Rudolf Siegert, the particles were morphologically similar to many “viruses,” including the rabies “virus” associated with the aforementioned Negri bodies. We can also find these filament-like forms associated with other “viruses” such as mumps, measles, parainfluenza, and many others.
According to Werner Slenczka, a man intimately involved in generating these EM images, the samples were contaminated by many microbial agents and even “paramyxoviruses” that made the interpretation difficult. He stated that the search for the “viral” particles was fatiguing and often frustrating. This confirms that the images used as evidence for the existence of the Marburg “virus” came from unpurified contaminated samples and thus there is no way to be able to state that the particles associated with the Marburg cases are in fact a “virus” at all. Slenczka also admitted that the monkeys assumed to be the source of the “virus” were never sick at any point and were used in other labs which never experienced any outbreaks whatsoever.
Even more interesting is that the attempts to “isolate” a “virus” were admitted to be failures. Early attempts to propagate the “virus” in cell cultures repeatedly ended in the lack of evidence of any “virus.” However, this did not stop researchers from trying numerous cell lines for culturing until they got the results they wanted to see. After successive trial-and-error resulting in confusing, conflicting, and contradictory results, it was decided that, while the Marburg “virus” could propagate in cell cultures, it did so without producing the cytopathogenic effect (CPE), the very criteria used by virologists to indirectly “see” that the “virus” has highjacked the cell in order to replicate.
What we are left with regarding the Marburg “virus” are non-specific symptoms of disease associated with non-specific Negri-like inclusions in tissues and particles claimed to be unique “viral” structures that are in fact morphologically similar to many other “viral” particles. We also have a “virus” that is said to propagate in cell culture while not producing the very effect looked for to determine a “virus” is present within the sample. In other words, the Marburg “virus” is yet another in a long line of names given to the same symptoms of disease represented by the same random particles. It is just another fraudulent theatrical production put forward by the pseudoscience known as virology.

The “Marlboro” Virus? I’m not impressed, much less convinced. There’s little here to distinguish this “Virus” from the rest of the family (of “packs”), which include; “Camel”, “Salem”, “Winston”, “Kent”, “Kool” etc.,and my personal favorite: “Viper”, as it reminds and demonstrates for us the obvious natural health benefits of “directly injecting toxins into the blood stream!
LikeLiked by 1 person
Sadly, they both succumbed to their symptoms after treatment at the hospital
LikeLike
Boris Johnson’s father chose this ‘virus’ to theme a novel originally called the Marburg Virus – now ‘the Virus’. He is seeking its republication.
A tweet I recently posted on Ukraine trauma is relevant to virus theory.
An inability to accept one’s own complicity in violent denial of others is masked in sacralising the ‘solutions’ set over projected hatred to ‘false flagged targets’ or scapegoats.
In simple, the virus serves as cover story for toxicity resulting from ‘technological progress’, such that vaccination and pharma are set heroically against a false flagged ‘threat’ to become itself a ‘sacred’ or unquestionable foundation from which and on which society and science must ‘grow’.
What we make sacred or special, we separate off from life as a god, idol or ideal to which life is then subjugated. There was no idea of progress in antiquity. But the first duty of the Pharaoh was to restore the (lost) Golden Age.
All the king’s horses and all the king’s men… applied to unifying a fragmentation of life.
LikeLiked by 1 person
Thank you….Fantastic-explanatory comment!
LikeLiked by 1 person
‘Undisclosed medication’ given is a likely culprit. This seems similar to the original Ebola outbreak (to be exact, the first one where it was ‘identified’).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2395567/
The funny thing is how they identify the actual culprit: “The index case in this outbreak had onset of symptoms on 1 September 1976, five days after receiving an injection of chloroquine for presumptive malaria […].
Within one week several other persons who had received injections at YMH also suffered from Ebola haemorrhagic fever, and almost all subsequent cases had either received injections at the hospital or had had close contact with another case.
[…] women 15-29 years of age had the highest incidence of disease, a phenomenon strongly related to attendance at prenatal and outpatient clinics at the hospital where they received injections.”
Of course they deflect to put the blame on the “virus”:
“The agent was isolated from the blood of 8 of 10 suspected cases using Vero cell cultures.”
Another funny find:
“Virus transmission was interrupted by stopping injections and by isolation of patients in their villages.”
If you look up Chloroquine side effects, even on wiki: https://en.wikipedia.org/wiki/Chloroquine#Side_effects
Among others there’s nausea, vomiting, diarrhea, shortness of breath, headache, confusion, muscle pain/weakness, leg/ankle swelling
There are a few more, but these ones are an EXACT match with early ebola symptoms. Also keep in mind that back then it was injected, not taken orally as is usual.
Nice work on the Marburg deception, Mike! Will you do an article on Ebola as well?
LikeLiked by 2 people
Spot on Rich! I believe these severe cases are indeed due to toxic treatments such as chloroquine. I was actually originally investigating Ebola but quickly realized that in order to do it justice, I needed to tackle Marburg first. Ebola is next on the list. 😉
LikeLike
Mike, a job well done. This is valuable information for anyone seeking the truth about Marburg, the manner in which it was said to be discovered, and the problems they claim should be of concern to society. Of course, the whole story is a fabrication, as you have aptly demonstrated, and in the end, they have the same thing they had in the beginning—nothing. I have noticed a pattern that is present in all their virus claims. Below is a rough outline of what I recognize.
Problem Phase
Symptoms
Origination
Contagion
Outbreak
Epidemic potential
Fatal (in some cases)
Verification Phase
Isolation (for proof of the virus)
Electron Micrographs
Experiments (studies and research work to determine the method of contagion)
Validation Phase
Papers (peer reviewed and published)
Official health agencies declare the level of emergency
Solution Phase
Governments and businesses follow health agency guidelines
Healthcare services follow guidance through protocols
Big Pharma readies medications
Compliance is required for solutions by governments and businesses
Controversy Phase
Censorship of dissent
Punitive action against professional rebellion and noncompliance
Termination Phase
Solutions exhausted
Level of emergency significantly reduced
Concern among the public wanes
The “virus” is shelved and added to the catalog of “viruses.”
LikeLiked by 1 person
Thanks George! That is a very good outline. You hit the major beats and the pattern for sure.
LikeLike
Mike,
Here is proof that we have entered what I called the Controversy Phase. This also marks the rise of the techno-fascist state.
California Will Now Punish Doctors For Refusing To Comply With The Establishment COVID Narrative
“Doctors and other medical professionals accused of spreading “disinformation” and “misinformation” can now have their state license suspended or revoked by the Medical Board or Osteopathic Medical Board of California for “unprofessional, conduct.”
The bill defines “misinformation” as: False information that is contradicted by contemporary scientific consensus contrary to the standard of care.
Note that it does not define misinformation as info that is contrary to scientific facts and evidence. Rather, it defines it as something that runs contrary to “consensus” and “standards of care.” The state government gets to dictate what the consensus is, and what the standard of care is. Meaning, any doctor that contradicts the STATE is subject to punishment. Science has nothing to do with it. . .’
https://www.zerohedge.com/covid-19/california-will-now-punish-doctors-refusing-comply-establishment-covid-narrative
LikeLiked by 1 person
This is well worth a listen. It is in remarkable agreement with the consensus on this website about the covid virus. It is thorough, logical, concise, and well presented by Dr. Poornima. It is incredible to find so much information in one video.
https://www.brighteon.com/01ac76d3-e9bc-4968-9abe-221f343ec9b6
LikeLike
https://apocalypticyoga.substack.com/p/the-sad-tale-of-poornima-wagh
The above generally aligns with my own sentiments.
Though I don’t engage in poor poormina.
The way in which we share is part of what we share.
I chose not to invest in her information after my first exposure – pending further clarity.
However we are all free to discern relevance and resonance according to our own ‘lights’.
LikeLiked by 2 people
I remember when Poornima paid us a visit. She didn’t stay very long after this savage sunk his teeth into her. Tasted like cardboard.
LikeLike
My guess is Poornima is CIA or something meant to discredit the anti-virus movement. I was skeptical of a few of her claims but overall I believed her because she seemed so sincere and genuine. I also wanted to believe what she said too.
A picture is worth a thousand words. Here’s a poster that explains the big picture of the Great Reset which I found in an Off-Guardian comment:
https://helpfreetheearth.com/News_1600/news1660_enemies.html
LikeLike
BTW I see the fear agenda working all sides or profiles to work a nocebo (self-destructive) effect – so her title is immediately out of line with my sense of constructive critical engagement in a complex issue.
“The Jab – It’s Poison And Will Kill You”.
Now some WANT this to be true. Others may FEAR it to be true, but I ask you who really knows?
LikeLiked by 1 person
Dr Merritt went well out of her way to interview Dr Poornima. Perhaps this video might clarify any areas of uncertainty concerning the information she presents.
https://article.wn.com/view-bitchute/2022/08/21/Dr_Lee_Merritt_interview_with_Poornima_Wagh_There_is_no_COVI/
LikeLike
I watched about half of the Lee Merrit interview… Coppolino is right when he refers to Wagh as “a dream come true — a scientific unicorn providing long sought-after vindication”… but so many cringe/uh-oh moments during the interviews I’ve watched with this lady… curious to see how this one unfolds.
“The London School of Hygiene and Tropical Medicine has checked in with the following statement this morning from their press office: “Nobody by the name of Poornima Wagh has obtained a degree from our institution.” We have also received a second confirmation from Roger Watson: “I have it from the dean of Faculty of Infectious and Tropical Diseases at LSHTM, Alison Grant, that nobody of her name has obtained any degree from their institution.”
That’s not a good look 😦
https://planetwavesfm.substack.com/p/charlatans-web
LikeLiked by 1 person
[audio src="https://audio.pwfm.tech/interviews/220826-1630-poornima.mp3" /]
Ugh!
LikeLiked by 1 person
Mike, how does one get in contact with you ‘off-list’? I can’t find any contact info or link for you on the website
LikeLike
My email is misto1481@hotmail. I’ve been getting quite a few emails recently and I do my best to respond to them as quickly as possible but I apologize in advance if it takes me a bit to respond.
LikeLike
Brought to you from Africa again? Less than 500 known cases over 55 years. Wow, what a super threat. It could be any severe reaction to some nasty toxin. It could be the result of some extreme lack of nutrients. For sure, if it was a virus floating around in the air, by now millions would have been infected. This is another fair tale created by virology mystique and fantasy. Man the barricades, hunker down and let the CDC save your soul once again.
LikeLiked by 1 person
FRAMING THE WORLD: THE DEBATE ABOUT VIRUSES WITH ANDREW KAUFMAN, M.D.
https://www.bitchute.com/video/7smX68fIi5QJ/
LikeLiked by 1 person
They never give up.
A new gene therapy based on antibody cells is about to be tested in humans
“During the covid-19 pandemic, antibodies played a front-and-center role. We used home tests to look for them, and we took vaccines so our bodies would make more.
Less attention was paid to B cells, the immune-system cells that actually make antibodies, churning out as many as 10,000 a second—and which, after an infection, can persist for years inside your bone marrow.
Now a biotechnology company based in Seattle says the US Food and Drug Administration has agreed to let it move forward with the first study in humans of a new type of gene therapy, using genetically engineered B cells. The company, Immusoft, plans to harness B cells to treat a rare inherited disease called MPS-1. . .”
https://www.technologyreview.com/2022/09/01/1058830/next-act-antibody-cells-new-form-of-gene-therapy/
LikeLiked by 1 person
How can ‘they’ give up?
They have to uplevel attack on life to ‘survive’ in a lie set over life.
‘They’ are the collective result of Our complicity & support for the ideas and intentions to lord it over life.
Are we on the verge of victory for the Ego writ large?
or the revelation of disclosure and replacement of a false basis for thinking, perception and identity in reaction?
LikeLiked by 1 person
“Are we on the verge of victory for the Ego writ large? or the revelation of disclosure and replacement of a false basis for thinking, perception and identity in reaction?”
Curiously, the ‘ultimate’ victory for the Ego leads to its own inevitable dissolution, so IMO both are kind of synonymous.
LikeLike
An example of vaccine propaganda:
Researchers study the long-term consequences of Finland’s first vaccine mandate against smallpox
“Researchers from University of Turku investigated how the vaccine mandate against the deadly childhood infection smallpox was successful at increasing vaccination coverage in 19th century Finland.
Poor vaccine uptake in vaccination campaigns limits vaccine impact on local and global health and compromises the health of at-risk individuals. . .”
https://www.news-medical.net/news/20220902/Researchers-study-the-long-term-consequences-of-Finlande28099s-first-vaccine-mandate-against-smallpox.aspx
LikeLiked by 1 person
Update.
I’m watching this one closely. It is a case of a legislative body abdicating their responsibility and passing their authority to make laws to technocrats. It is the duty of the legislative body to consider all the facts and not defer judgment to the consensus of technocrats. It is therefore fascist because the state will merge with an unelected entity to violate the constitutional rights of the people.
California Passes Bill To Criminalize Dissent of Covid-19 Narrative
“A California Assembly bill that will criminalize dissent of Covid-19 narrative by requiring the Medical Board of California to punish licensed doctors who “disseminate misinformation or disinformation related to COVID-19” has passed through the state Senate and is now headed to the governor’s desk. . .
. . . According to the bill, “misinformation,” is “false information that is contradicted by contemporary scientific consensus contrary to the standard of care.” The bill defines “disinformation” as “misinformation that the licensee deliberately disseminated with malicious intent or an intent to mislead . . .”
https://newspunch.com/california-passes-bill-to-criminalize-dissent-of-covid-19-narrative/
LikeLiked by 1 person
It’s just a misdirection play, George, in order to set-up the problem (OT Capitalism culture) that (literally and figuratively) lies in service of the reaction (broad-spectrum antifascism from the Right, the Left, and the Independents) which, itself lies (literally and figuratively) in service of the solution that is the coming national socialist wave of culture change, which is the Third Way anticapitalist sociopolitics best structured to manage collapse.
Let’s try not to be part of the reaction in service of the solution as if we were a political sucker born again every hour.
LikeLike
These frankencells are artifactual and will soon succumb to the rolling blackouts. It’s only natural that ‘peak separate-selfhood’ would result in ‘peak biohacking,’ to put it euphemistically. We all know what it is to try and paper over our shortcomings with inappropriate cheats. That’s civilization for you. That’s what our ancestors who waved the white flag subjected us to. And what, in domestication, we continue to subject ourselves to in order to not be a street scavenger, in prison, or dead.
But now that we can clearly see that Collapse is knocking on the door, we can forgive ourselves for our current self-subjugation because open ecological spaces await those who are prepared to move through the gauntlet and into them – in a return to creational living.
An enslaved mind is a lost cause but a slave’s mind is a terrible thing to waste on missed opportunities to move towards the true freedom of living on Earth as Earth peoples, which is the only ‘game’ there is and ever was.
It’s also only natural that at ‘peak separate-selfhood’ few can handle that type of responsibility which, again, begins with the body. Get your body that wants to get back to true, back towards true. The mind is just a thinky consideration for considerate holography, and nothing more. The body is our mother consciousness. Truing the body mostly revolves around diet. Once the body is well on its way towards true the mind will automatically be drawn, by the body, to the land and that is the beginning of the ego death. It happened to me. It obviously happened to Clarifire who is making the move back to the land as we speak.
It generally begins by finding a local food club or other farmer-direct food source of organic grassfed foods, and going through a loading phase. Clarifire would say it best begins with a long fast and I believe him. Going barefoot at all times except when you need protection also helps, in more ways than just energetic. If you’re not allowed somewhere because you don’t have shoes on then it reinforces the fact that you don’t belong there. The shoes become shackles in a very real sense, and being a barefoot person becomes a strong mental (and physical) aid in combatting one’s separate-selfhood. Once you’re back out on the land and strong again you might find that you shod yourself more often than you did the easy streets of asphalt and concrete, because the work on that next level calls for it. It all depends on the terrain.
LikeLike
Our being is designed to heal itself if you remove or limit harmful factors of an emotional-sentimental, chemical, pharmaceutical, electromagnetic and climatic nature and if you conserve vital energy through physical and intellectual relaxation, sleep, weather protection and nutrition proper. In this consists all True Medicine, all the Art of Healing.
Yes, our being was created with bio-energetic programs for automatic adaptation to harmful factors, rebalancing of vital energy flows, detoxification, waste elimination and tissue regeneration. He who claims that through his so-called medical science he succeeds in healing is either a stupid and vain ignoramus or an unscrupulous swindler.
LikeLike
He who claims that through his so-called medical science he succeeds in curing the sick is either a foolish and vain ignoramus, or an unscrupulous swindler.
LikeLike
Medical care has helped my acne, busted knees with partial knee replacements, dental work, and pain associated with kidney stones…others. Are these “cures”?, well depends on the definition, they are greatly improved but not completely resolved problems..and none are related to viruses. So while we are on the same side, dont throw out the baby with the bath water.
LikeLike
The “Experts” Still Aren’t Giving Up on Vaccine Mandates
“Dr. Gilbert Berdine of the Texas Tech University Health Sciences Center and Ryan McMaken discuss the policy makers’ justifications for vaccine mandates over the past two years. . .
. . .It is very risky for anyone in the medical community to criticize any aspect of covid policy. This includes mask policy, alternative therapies, vaccine mandates, or quarantines. Licensing boards, including the American Board of Internal Medicine, have threatened physicians with the loss of licensure for spreading “disinformation” about covid-19. Of course, disinformation has nothing to do with correct or incorrect information, but rather means anything that contradicts a political narrative. The practice of medicine is gradually being transformed from a scientific inquiry seeking fact into a religious cult accepting dogma under the threat of excommunication. . .”
https://mises.org/wire/experts-still-arent-giving-vaccine-mandates
LikeLike
THE NEXT VAX: Big Pharma pushing to release ANOTHER mRNA “vaccine,” this one for RSV (respiratory syncytial virus)
“After seeing the success, aka dollar signs, of the Wuhan coronavirus (Covid-19) “vaccine” rollout, the pharmaceutical industry – and specifically Moderna – is now setting its sights on a new mRNA (messenger RNA) injection for respiratory syncytial virus, also known as RSV. . .
. . .“Second only to the flu when it comes to causing significant respiratory illness in adults, RSV represents an often unrecognized yet very real and imminent threat to our older population,” says Michael Clay, Javara’s Chief Operation Officer. “Being able to vaccinate against this virus would save lives, prevent hospitalizations, and conserve healthcare resources.”. . .
. . .Moderna says its new RSV jab candidate contains the exact same mRNA technology as the company’s Fauci Flu shots, which are linked to myocarditis and a host of other deadly conditions. . .
. . .“We have observed in preclinical results a very strong immune response against all the antigens,” Ceddia claimed in an interview. “That’s another important feature of mRNA vaccines, particularly our mRNA platform, which allows for including more and more antigens in combination.”. . .
(This is a fraudulent statement because there are no molecular structures on the surface of the virus to act as antigens because there is no virus. The mRNA in the “vaccine” cannot therefore produce a synthetic protein to act as an antigen when there is no antigen in the first place. Furthermore, there is no evidence that ribosomes can be hacked by mRNA to produce proteins of any kind. The so-called immune response is really an inflammatory response to the adjuvants in the injection and to the payload of whatever is in the nanoparticles, if there is anything in them at all, and to the nanoparticles themselves.)
. . .In the future, Ceddia added, a person will be able to go to the pharmacy and receive one shot containing all of Moderna’s mRNA drugs. This will be especially appealing for children, she says, as parents will no longer have to return for multiple different shots as part of a schedule.” . . .
https://vaccines.news/2022-09-02-pharma-mrna-vaccine-rsv-respiratory-syncytial-virus.html#
My God, what madness!
______________
Isolation and Characterization of Clinical RSV Isolates in Belgium during the Winters of 2016–2018
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6893609/
LikeLiked by 1 person
Re-read this after these months due to “Marburg” heading up by WHO. Great article here by Mike, seems time to take an extract and put it on a few platforms.
About mRNA, seems no one has found much if any mRNA in the shots nor do they seem to make spike protein because there is no paper on mRNA-Spike dose response. I guess it’s a cover for graphene and LNPs.
LikeLiked by 1 person
I found something on EMF, DNA as fractal antenna and stress protein.
with an image of the relevant study text.
LikeLike
She believes in prion proteins (which are a cover for insecticide toxicity) the virus attaching to ACE receptors, spike proteins, exosomes (do exist but don’t infect) infecting the whole body–no proof of any of these concepts has been found. She even smirks when talking about this happening to people. This is a cover for the graphene and LNP for which there is lots of evidence.
LikeLike
As I don’t accept the virus of reconstructed fragments, I cant accept spike protein as anything but GoF running on virus operating system. Any invested/believed narrative can run as a program through which other variations and spinoffs are generated. But from the POV of the one whoi masks from feared/hated reality, the program runs to defend against disclosure. Nanotech is also a huge investment seeking returns. So the sales pitch likewise will be PR mixed with partial truths taken out of context.
>
LikeLiked by 1 person
To briansteere, good points. Just to point out there can’t be a viral op system because there is no virus in nature every found so you wouldn’ t be making a virus, perhaps a LNP with some functions but not enough to be replication competent and have all the so-called virus functions as that is too complex and only theoretical. About Spike, the drug co MUST have done a pre-clinical pharmacology dose-response study to show mRNA making spike if the mRNA to spike is true. Since there is no such study, nor a purified spike study, it seem like no mRNA, no spike is a clear possibility and I wouldn’t put it past them to make a story about the vax since that’s what they did about the virus.
LikeLiked by 1 person
The belief in a virus (as sold) is all that is needed for dark GoF ‘research. The viral nature of a psyop is evidently contagious – pause before reacting or you only demonstrate the ‘mechanism’ that allows them to run. Most assume mRNA does what it is said, invested in and sold to do – transfect cells to force-replicate proteins to order. So accepting the virus idea as a manual intervention.
The bio-markers for ’spike P’ are indeed linked to ’something or things’ that are not investigated because experts tell us what they are – within a wrapping of hight tech Big Science – so they MUST know – eh? A premise to test ius if a particular stress protein results from new emf exposures. Flagging this onto a mass mRNA spike rollout might be another covers story to use as a basis to build on. That’s how they are protected – by basing social order on their premises, so to become too big to fail – like tares in the crop in the Bible story.
>
LikeLiked by 1 person
There are a certain number of harmful factors (exhausting, toxic, harmful) that affect our whole being with an emphasis on different compartments of it… and, consequently, there are self-healing processes that consist in the adaptation of vital energy flows, functions and tissue structure for survival. This is the definition of what people call “disease”.
LikeLike
There is NO money to be made in health if you are trying to sell real knowledge to the masses, expressed so simply and clearly that it is accessible to anyone’s understanding. Money is only made in health if, while you pretend to explain to people about illness and health, in reality you keep them in that ignorance that generates the fear of illness and death… while you sell them consultations , investigations, drugs, vaccines, procedures and purported natural remedies and supplements. This is how much money is made in “medicine”… by no means explaining to people in words and in ordinary terms what the disease state is and what they can actually do to promote the natural processes of self-healing.
LikeLike
Yes, it’s about money, and power, and control, and much more. It was also the subject of prophecy.
“. . . If you put the original Greek word “pharmakeia” in place of the English word “sorceries” the end of verse 23 would say, “For by thy pharmakeia were ALL nations deceived”! “Pharmakeia” is where we get our English word “pharmacy”! Pharmacy is a well organized and professionalized system that administers poisonous drugs. The Bible reveals that Babylon will deceive all nations by the use of pharmacy that is in connection to “magical arts” and idolatry. . .”
https://www.pathwaytopeace.net/index.php/blogs-and-articles/pharmakeia-deception
LikeLike
Perhaps we should study this further. the Bible had a Greek translation, not origin.
But I understood poison and cure to be both implicit in the term.
Without some sense of the symbolic and associative mind of the ancients, we project our rationally premised world onto theirs and mistranslate everything – as the process of cultural mutations.
The usurpation of Religion (as the Way or living Cultural expression of a people) by magic is the taking of Reality (God/Creation) in iMage as a false object model, introducing a middleman into the temple – which is consecrated by its devotions and not made of stones.
Living religion is formless and indivisible in the heart, and so ‘organised religion’ is a structure set over life to which we are sacrificed that the structure survives, that was invoked in conflict and chaos to ‘make us safe’ from fear of truth as Retribution. Hence the supplications to God or Gods of terror for appeasement – which sought a mitigation of total sacrifice by bargaining – that was set by an emergent priesthood to adjudicate or administer.
The mindset in sympathies and similars uses the forms and images of symbolic relevance as an energetic attunement.
That the remedy is where the problem is, is magically concealed by hiding it in a false ‘solution’. The process of cultural mutations can be seen as layers of masking over unhealed conflicts by which to ‘run out of space and time’.
But to truly address a conflict is to release the cultural baggage by which we presume to see and know, so as to see with new eyes. yet the willingness to see has to persist through every psychic-emotional defence against seeing, because we have learned, adapted and been trained to see what our minds are predicated to see as our protectors from truth for which we are not ready or willing to accept..
I think many here will recognise the magical thinking of false solutions, whether as a market demand or a marketeering of would-be ‘saviours’ seeking a booster for their image.
Another name for God is Source. The Word that proceeds from Source is that by which all that is knows itself as all that is. But as creators we are free to filter, augment, shape and colour our extensions of all that is, and by taking what we make as true in itself, mistake image and symbol of Self and world for the living Communication of being by which we are.
That sorcerers become trapped in their own mis-creations is also that casting out from heaven finds us cast out, rejected, denied and sorely oppressed!
The law of giving and receiving is not applied externally – yet that is what our ‘externalised’ thinking takes on as the attempt to manage and control a Life we have forgotten how to truly receive, appreciate and discern.
LikeLike
Reading through this article, I was struck by the fact that there seems to be no activity from these “highly infectious” viruses then, all of a sudden, an outbreak here, another outbreak there.
If these pathogens were so infectious, there should be constant outbreaks everywhere. Why don’t we see that? Are we so good at managing these viruses that we only see outbreaks when we drop our guard or get lazy?
I’ve heard that, compared to respiratory viruses, things like Ebola and Marburg are very difficult to catch but more uniformly fatal than the flu, etc.
Looks like we’re not going to run out of things to worry about anytime soon.
LikeLiked by 1 person
Hi Antonio,
Sorry it took a while to respond. It is definitely odd how these diseases just pop up and disappear randomly. I wonder where the “viruses” go when the outbreaks subside… 🤔
LikeLike
Did you read Hope Simpson’s The Transmission of Influenza?
The early chapters are very interesting on the lack of acceptance for the ‘virus’ idea UNTIL the electron microscope ‘enabled its discovery’. Which pushed most to abandon open critique.
BUT he so extensively studied the epidemiology of outbreaks as to defy logical supposition of direct contagion, so as to propose a dormancy that was re-activated by temperature (possibly also atmospheric conditions – ie moisture levels – I cant recall.
I can forward a ref copy.
Opening chapter heads:
Chapter 1 The Scope and Purpose of the Book.
Antiquity of the Doubt that Influenza Is Contagious
Theophilus Thompson’s Anthology
Dubiety despite Advance in Knowledge
Personal Involvement in the Problems of Epidemic Influenza
Deficiency of the Current Concept: The Influence of Season
The New Concept of Virus Persistence, Latency, and Seasonal Reactivation
Other Alternative Hypotheses
The Importance of the History of the Behavior of Human Influenza Viruses
Chapter 2 The Debate about the Contagiousness of Influenza
The Ubiquity of Influenza
An Influenza Epidemic in the Seventeenth Century
Ideas about Influenza in the Eighteenth Century
The Nineteenth Century before Pasteur
Opinion in the Nineteenth Century after Pasteur
Chapter 3 Epidemic Influenza, 1900-1932
1900-1916
Prelude to the 1918 Pandemic.
ThePandemicof 1918
1919-1928
1928-1933
Chapter 4 The Effect of the Discovery of the Causal Organism.
The Discovery of an Influenza Virus
The Discovery ofa Human Influenza Virus
The Influenza of 1932-33 in a General Practice
The Conceptual Impact of Discovery of the Influenza Viruses
Field Studies that Stimulated New Ideas
Transequatorial Swing ofInfluenza
The Role of Herd Immunity
A New Hypothesis from Andrewes
The Vanishing Trick
LikeLiked by 1 person
It’s because the names of these “viruses” are the same as “Godzilla”. They are a registration in a screenplay, not an actual object. When one episode of Godzilla is over there is no more Godzilla until the next episode.
LikeLiked by 1 person
Mike, – the “virus” cultists are spreading fear porn again, – see https://www.youtube.com/results?search_query=nipah+outbreak+in+kerala&sp=EgIIBQ%253D%253D
These cultists have long tasted blood and won’t stop.
Those who have woken up to their fraud can fight better if there is specific ‘ammunition’ to challenge this latest nonsense.
Hence, if you or others in your circle of acquaintances haven’t already done so, consider citing and then pointing out the flaws in the original “scientific” articles which started the “nipah” bandwagon and poking holes in that deception / delusion.
.
LikeLiked by 1 person
Mike, kudos for the new post on nipah! Notably, the cultists pat themselves on the back for being able to “contain” the “spread” of the unicorn. https://www.youtube.com/watch?v=-ATwOaiRszc
It looks like they can now regularly pull off these pseudo-health scares and claim credit for ‘controlling’ the ‘disease’. Besides being used for mind-control / brain-washing, such ‘outbreaks’ are convenient excuses to silently push through power-grabs – https://rumble.com/v3lvfm4-sinister-who-plans.html
And if cornered, they can always claim the unicorn has ‘mutated’ – https://www.youtube.com/watch?v=g92m2bw6Nh8 – perhaps into a non-‘deadly’ avatar!
LikeLiked by 1 person
You may have heard of talk of a ‘cyber pandemic.’
Which, if as cooked up / deviously ‘set off’ like ‘Co(n)vid’, can be a convenient opportunity to also limit the reach of, if not silence, pesky ‘heretics’.
So, to reiterate one other suggestion, Mike, – and please remind the others in your circles too, – viz.,
Have backup copies of ALL your work/articles/videos and store them OFFLINE at safe, secure locations (ideally plural).
You don’t want to wake up one day to notice that your valuable efforts have been quietly wiped out / ‘memory-holed’.
LikeLike