
Due to the media hype of the “Tripledemic” (previously known as the “Twindemic”), most are probably well aware and fairly familiar with the name “respiratory syncytial virus,” otherwise known as “RSV.” We’ve been warned over the last few months that there was an alarming increase in cases of this “virus,” primarily amongst children, and that it was adding to an escalating burden on our healthcare system along with “Covid” and “influenza.” Obviously, as “RSV” is said to attack primarily infants, it has set concerned parents off into a panicked hysteria over how best to protect their children from yet another “virus” floating in the increasingly “viral-filled” air. However, is it necessary to be alarmed at the mere mention of the threat of “RSV” or is this yet another in a long line of media-hyped figments of the imagination? As I’ve covered “SARS-COV-2” and “influenza” quite a bit, it’s time to set the sights on “RSV” and see what kind of scientific evidence they have in store for us in order to justify this supposed “threat.”
To begin with, what exactly is RSV? What symptoms are we potentially dealing with here that set this “virus” apart from the two that are said to be currently causing mayhem around the world? Let’s take a look at a CDC list of the common symptoms between “RSV,” “Covid,” and “influenza” and see what distinguishes the “viruses” from one another:
It looks like the symptoms match up to a T beyond the regularity of occurrence. From the article accompanying the image, we get some more information regarding whether these “viruses” can be distinguished based upon symptoms alone:
Suffering from flu, RSV or COVID-19? How you can tell the difference
The three viruses have many symptoms that are similar.
“All three viruses have symptoms that are similar, which can make them difficult to tell apart. But knowing which virus a person has can help them receive proper treatment or, if need be, let them know if they need to isolate.”
“COVID-19, flu and RSV are more similar to each other than they are different in terms of symptoms.”
“However, public health experts told ABC News the absence of one of the symptoms does not mean a patient doesn’t have a particular virus and that the only way to be sure is to get tested.”
“In most cases, if anybody has generic symptoms, such as fever, cough, runny nose, there’s going to be no real way to distinguish which one is which without a test,” Dr. Scott Roberts, an assistant professor and the associate medical director of infection prevention at Yale School of Medicine, told ABC News.”
According to the list provided by the CDC, it looks as if every single symptom is shared between all three “viruses.” The only difference is claimed to be in regards to the regularity of a particular symptom occurring. However, it is stated that even the absence of a particular symptom can not rule in or out any of the “viruses” and that testing is necessary in order to obtain a definitive diagnosis. Thus, it is clear that there is no way to clinically diagnose any of these “viruses” by way of symptoms alone. I dealt with the problem of differential diagnosis in an article at my Substack.
The CDC confirms that the symptoms associated with RSV are nonspecific and overlap with many “viral” and bacterial diseases. As clinical diagnosis based on symptoms alone is impossible, the testing that is used to identify “RSV” is the usual culprits with PCR and antigen tests. “Viral” culture and antibody tests are said to be less commonly used with antibody testing limited to research and surveillance:
Clinical Laboratory Testing
“Clinical symptoms of RSV are nonspecific and can overlap with other viral respiratory infections, as well as some bacterial infections. Several types of laboratory tests are available for confirming RSV infection. These tests may be performed on upper and lower respiratory specimens.
The most commonly used types of RSV clinical laboratory tests are
- Real-time reverse transcriptase-polymerase chain reaction (rRT-PCR), which is more sensitive than culture and antigen testing
- Antigen testing, which is highly sensitive in children but not sensitive in adults
Less commonly used tests include:
- Viral culture
- Serology, which is usually only used for research and surveillance studies
Some tests can differentiate between RSV subtypes (A and B), but the clinical significance of these subtypes is unclear. Consult your laboratorian for information on what type of respiratory specimen is most appropriate to use.”
https://www.cdc.gov/rsv/clinical/index.html
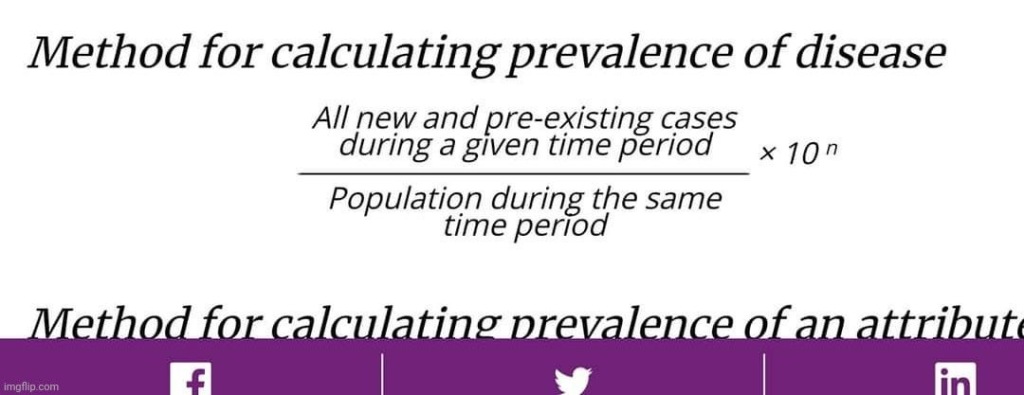
However, there is a major problem with relying on these tests to diagnose cases of a particular disease. As “RSV” can not be accurately diagnosed clinically due to nonspecific and overlapping symptoms, there is no way to identify cases in order to determine the prevalence of the disease within a given population. In order for the results of the PCR test to be considered accurate, disease prevalence must be known first. As defined by the CDC, prevalence is “the proportion of persons in a population who have a particular disease or attribute at a specified point in time or over a specified period of time.” This is how the CDC calculates disease prevalence:
Disease prevalence of “RSV” can only be determined through cases identified by clinical diagnosis, which the CDC admits is an impossibility due to the nonspecific and overlapping symptoms. There is no way to distinguish “RSV” from “Covid” nor the “flu.” As the PCR test results are unable to be interpreted accurately without establishing disease prevalence first, the PCR test is useless as a diagnostic tool. Thus, the health institutions are creating cases of “RSV,” “Covid,” and the “flu” through PCR testing in order to claim the legitimacy of the PCR results used to generate the cases. This is obviously fraudulent and illogical circular reasoning as the test itself can not be used to create the cases needed in order to determine a disease prevalence rate used to legitimize the results of the test.
It is clear to see for anyone looking at this situation both critically and logically that the same symptoms of disease have been given numerous names associated with various “viruses” over the decades. The rise and reliance on molecular testing to distinguish between these “viruses” is a recent phenomenon that can only be valid if the “viruses” being tested for were purified and isolated directly from the fluids of a sick host and proven pathogenic in a natural way to begin with. However, this has never once been done once for any of these “viruses” and it will be seen that it is no different for “RSV.” Let’s take a quick peek at the story provided for the discovery of this “virus” before diving in-depth into the papers supplied as evidence:
History
“RSV was discovered in 1956 but was not initially associated with respiratory illness among infants. Indeed, when a group of 14 chimpanzees were noted to be suffering from colds and coryza, Morris and co-workers isolated a new virus originally named chimpanzee coryza agent (CCA). Subsequently, Chanock and co-workers confirmed that the agent caused respiratory illness in humans when they obtained isolates from two children, one with laryngotracheobronchitis and the other with bronchopneumonia, that were indistinguishable from CCA. When specific neutralizing antibody to CCA was found to be present in most school-aged children, “chimpanzee coryza agent” was more appropriately renamed respiratory syncytial virus to denote its clinical and laboratory manifestations.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7173590/
As can be seen from the above passage, “RSV” was originally discovered in 1956 by Morris et al. in chimpanzees, not in children. It wasn’t until a year later that Chanock et al. “confirmed” that the chimpanzee coryza agent (CCA) was capable of “infecting” humans based off of “isolates” obtained from two children. However, is this story true? Did either team really isolate a new “virus” which was found in both chimpanzees and humans that was capable of producing respiratory disease? Was a “virus” actually properly purified and isolated directly from the fluids of a sick host and subsequently proven pathogenic in a natural way? Were proper controls carried out for any of the experiments performed and what, if anything, did they show? Let’s examine these questions and more by looking at the three papers supplied as the evidence for the discovery of “RSV.” I am presenting the entirety of the Morris et al. 1956 paper as well as the first paper in 1957 from Chanock et al. I edited out some of the antibody experimentation from a follow-up study by Chanock et al., also from 1957, for length consideration and because the information was redundant. All three papers are available for download or to look up via the DOI number. To break down the evidence for “RSV,” I am trying a different format where I am providing commentary throughout the study rather than summarizing important points beforehand. Let me know in the comments if you prefer one way over the other.
Recovery of Cytopathogenic Agent from Chimpanzees with Coryza.
Right off the bat, we can see that Morris et al. did not seem wildly confident in their discovery as they described the “virus” as being of “apparent” (i.e. seeming to be real or true, but not necessarily so) etiologic significance. They claimed to have established an association between the agent and respiratory illness in a lab worker but then admit that the serological evidence suggested that it could either be the agent that they “discovered” or one that was closely related.
During October, 1955: a respiratory illness characterized by coughing, sneezing and mucopurulent nasal discharge occurred in a colony of 20 “normal” chimpanzees at the Walter Reed Army Institute of Research. The present paper describes the isolation of a virus of apparent etiologic significance in the epizootic, establishes an etiologic association between the chimpanzee coryza agent and respiratory illness in a laboratory worker and finally, presents serologic data suggesting that a number of human beings have experienced infection with the chimpanzee coryza virus or an agent closely related to it.
The materials used for the “isolation” of the “virus” were throat swab samples from 14 of 20 young monkeys said to be clinically ill with coryza, a catarrhal inflammation of the mucous membrane in the nose. A group of older monkeys, which had been previously experimented on for human hepatitis “virus,” were used in transmissibility experiments. This invalidates the monkeys as a proper control. The “virus” was grown in tissue cultures which consisted of epithelial-like cells derived from human liver that were incubated in roller tubes with nutrient medium consisting of Eagle’s basal medium, inactivated horse serum, and L-glutamine. Penicillin and streptomycin were added to control adventitious bacterial contaminants.
Matcrials and methods. Chimpanzees and collection of specimens. The chimpanzees in the epizootic were 15 to 20 months old and were obtained from a commercial breeder in Dania. Fla., 3 to 24 weeks prior to their illness. They were housed at the Forest Glen Annex of the Walter Reed Army Institute of Research (WRAIR). Blood specimens for serological study were obtained from individual chimpanzees at outset of the epizootic on Oct. 13. 1955, when 5 of the 20 animals were suffering from clinical coryza, and periodically thereafter until Apr. 18. 1956. Throat swabs
were obtained from all animals in the colony on Oct. 17. 1955 when 14 of the 20 animals were clinically ill with coryza; the swabs provided the material employed for viral isolation studies. Another group of somewhat older chimpanzees was used in studying experimental transmissibility of the coryza. The 6 animals in this group had been inoculated previously with material presumed to contain the virus of human infectious hepatitis: they were housed in a different location from the others and had had no direct contact with other chimpanzees for over a year.
Tissue cultures. Cultures of epithelial-like cells derived from human liver (Chang strain) were prepared by the method of Chang(1). The cultures were grown in roller tubes (1.5 x 13 cm) and stationary bottles (4 x 4 x 14 cm) in nutrient medium consisting of 8 parts Eagle’s basal medium (2), 2 parts inactivated horse serum, and 0.2 part L-glutamine. Penicillin (100 uniits/ml) and streptomycin (20 ug/ml) were added to control adventitious bacterial contaminants. Tubes and bottles contained 1 ml and 15 ml of nutrient fluid, respectively. The cells were fed on the 3rd or 4th day by replacing the old nutrient. fluid with an equal amount of fresh nutrient. Cultures were incubated at 36°C and at the time of use were usually 4 to 6 days old.
The “virus” was said to be “isolated” from the throat swab specimens in 1 out of the 14 monkeys. The sample was immediately rinsed in nutrient fluid containing antibiotics and then centrifuged for a bit to remove larger particles. At no point was the sample ever checked by electron microscopy for evidence of the assumed “viral” particles within the sample before it was added to either the nutrient fluid or the tissue culture. In fact, there are zero EM images of the supposed “virus” in any of the three papers presented, even after the cell culture experiments were performed. After 4 days of incubation, the fluids were replaced with fresh nutrients/antibiotics, which resulted in the death of the cells and signs of the cytopathogenic effect 4 days later. None of the samples from the 13 remaining monkeys resulted in the same cytopathogenic effects.
Isolation of coryza agent. A fresh (witthin the hour of collection) throat swab from a chimpanzee (Sue) involved in the epizootic was washed in 2 ml of tissue culture nutrient fluid containing antibiotics. After centrifugation at 3000 rpm for 15 minutes to remove large particles, 0.2 ml of the supernatant was inoculated into a roller tube culture of 4-day-old Chang liver cells. After 4 days incubation the original cell nutrient was replaced with fresh nutrient. Four days later cellular degeneration characterized by rounding, granulation, and sloughing from the tube wall was noted. Serial transmission of the cytopathogenic agent to other tube- or bottle-cultures of Chang liver cells was readily
accomplished by passage of suspensions of degenerated cells in their infected fluids. Simlilar isolation attempts which were made with materials obtained on October 17th from 13 other ill chimpanzees gave negative results.
I am glossing over the antibody results, which are nothing but nonspecific chemical reactions stemming from, in this instance, the mixture of human and horse blood. In order for antibody results to have any meaning, antibodies and the antigens themselves must be properly purified and isolated along with the assumed “viral” particles. As this has never occurred once in either case, it is impossible to use results obtained from one invisible hypothetical entity to indirectly claim the presence of another invisible hypothetical entity.
Serologic procedures. Virus. Seed virus was obtained by inoculating bottles of liver cells with the chimpanzee coryza agent (CCA) and harvesting cells and fluids 8 davs later when the infected cells characteristically showed complete degeneration. After grinding in a TenBroeck grinder the mixture was clarified by centrifugation at 3000 rpm for 15 minutes. The resulting supernatant constituted the seed vilrus. Infectivity was preserved by storage at -70° tin sealed glass ampoules.
Neutralization tests. Serial 2-fold dilutions of serum which had been inactivated at 56° for 30 minutes (0.15 ml) were mixed with a constant amount of virus (100 to 1000 tissue culture LD50) contained in 0.15 ml of infected tissue culture material. The mixtures were incubated in a water bath at 37°C for 1 hour after which 0.1 ml of each mixture was added to each of 2 tubes containing normal liver cells. The cultures were examined microscopically for cellular degeneration after a 6- to 8-day incubation period. The neutralization titer was considered the highest dilution of serum completely inhibiting cellular degeneration. Appropriate cell and serum controls and a virus titration were included in each test.
Complement fixation tests. Satisfactory complement fixing antigen was prepared from infected liver cells grown in medium containing 20% inactivated horse serum. When the horse serum component of the medium was not heated at 56° for
1/2 hour the material was anticomplementary if used in the complement fixation (CF) procedure employing overnight fixation in the cold, in accordance with the standard technic of the Department of Virus Diseases, WRAIR (3) which was used in the current studies. For use in CF tests human and chimpanzee sera were inactivated for 30 minutes at 56°C and 60″C, respectively. The serum titer was expressed as the reciprocal of the highest dilution giving 75% or greater fixation of complement after overnight incubation at 4°C in the presence of 2 units of antigen and 2 full units of complement. Controls included in each test were antigen (prepared from uninfected liver cell culltures propagated in inactivated horse serum), positive serum (obtained from a man who experienced a labratory infection, patient B1 in Text Fig. 1, and saline.
The next two sections are rather revealing. In the inoculated culture taken from the sample of one monkey, the cytopathogenic effect was observed after 8 days, and inclusion-like bodies were noted in the liver cell cultures. Inclusion-like bodies are defined as “aggregates of virus particles or virus-induced proteins or special structures characteristic of infection by viruses either in the cytoplasm or the nucleus.” Thus, these effects are supposed to be specific to “viruses.” However, the exact same inclusion-like bodies were observed in the uninoculated control cultures showing that the presence of an imaginary “virus” was unnecessary for this nonspecific effect to occur. Sadly, this damning information did not faze Morris et al. as they continued to believe that they had a new “virus.”
However, if this information was not damaging enough to their conclusions, the attempts to prove pathogenicity should have sunk their battleship entirely. The researchers attempted intracerebral and intraperitoneal inoculations into one-day-old mice, weanling hamsters and young adult rabbits and guinea pigs. They intranasally inoculated 8 to 10 gram mice, young adult rats, and 16 to 20 lb chimpanzees. Groups of chick embryos (7 to 11 days old) were inoculated on the choriolallantoic membrane and into the amnionic, allantoic and yolk sacs. None of the inoculated animals or embryonated eggs, other than chimpanzees, developed signs of disease during observation. The one exception was a single guinea pig that developed a persistent fever beginning on the 3rd day, but this was eventually declared to be bacterial in nature. On top of this lack of pathogenicity, the cytopathogenic effect observed differed based upon the cell line used during culturing. When monkey kidney cells were used, the CPE obtained was difficult to interpret because of the presence in the cultures of adventitious simian “viruses.” These are the same invisible foamy agents said to produce CPE in uninoculated cultures as observed by Enders, Rustigian, Cohen, Von Magnus, and Hull. Thus, this is yet another study supplying evidence that cell cultures and the cytopathogenic effect are an invalid and unreliable method to determine the presence of any “virus.”
Results. Behavior of chimpanzee coryza agent (CCA) in liver cell culture. Inoculation of CCA obtained from the culture of the throat swab of chimpanzee Sue into liver cell cultures produced little or no change during the first 5 or 6 days. On about the 7th day scattered islands of round and granular cells appeared and a few cells were disintegrated and dislodged from the glass wall of the container. Once begun, the process of degeneration spread rapidly and within 24 hours practically all cells were dead and some were floating in the nutrient fluid. Intranuclear and intracytoplasmic inclusions which are eosinophilic in Giemsa-stained cell preparations, were observed in culltures of liver cells infected with CCA. However, similar inclusion-like bodies were demonstrated in uninoculated cells, grown in inactivated horse serum. At the present time the significance of the inclusion-like structures found in infected and uninfected cells cannot be stated with certainty.
Pathogenicity of CCA for laboratory hosts. Tissue culture materials containing 100 to 10,000 TC LD50 of CCA were inoculated by the intracerebral and intraperitoneal routes into one-day-old mice, weanling hamsters and young adult rabbits and guinea pigs. Other 8 to 10 gram mice, young adult rats and 16 to 20 lb chimpanzees were inoculated intranasally. Groups of chick embryos (7 to 11 days old) were inoculated on the choriolallantoic membrane and into the amnionic, allantoic and yolk sacs. With the exception of a single guinea pig that developed persistent fever beginning on the 3rd day, none of the inoculated animals or embryonated eggs other than chimpanzees developed signs of disease during observation periods ranging up to 28 days. The etiology of fever in the guinea pig was ultimately traced to a bacterial infection. Further, the fluids obtained from chick embryos inoculated by various routes failed to agglutinate chicken and human “0” erythrocytes. Tube cultures of human cells derived from conjunctiva (Chang) , intestine (Henle) and human embryo fibroblasts (otbtained from Microbiological Associates) were found to be less susceptible to the cytopathogenic effect of CCA than liver cells; these cells showed only incomplete degeneration after 16 days incubation. Monkey kidney cells underwent complete degeneration 8 days after infection with CCA but the cytopathogenic effect obtained was sometimes difficult to interpret because of occasional presence in the cultures of adventitious simian viruses (4).
Once again, unreliable antibody results were utilized to claim a relation between animals said to be stricken with the same imaginary “virus.” Even when healthy animals developed a rise in antibodies, they were assumed to have had the “virus” even though there was zero evidence that the animals were ever sick. In the healthy animals, which showed neither illness nor antibody rises, it was assumed that they had no contact with the “virus.” There is always an escape clause available for unfavorable findings.

Relation of CCA to epizootic coryza in chimpanzees at Forest Glen. CCA was found to be related to the epizootic disease of chimpanzees at the Forest Glen Annex of the WRAIR by the use of serologic technics. Illustrative results of CF and neutralization tests performed on sera from 2 of the chimpanzees in the Forest Glen epizootic are shown in Table I. It is seen that in both animals CF antibody against CCA was undetectable in the early sera but titered 1:40 or 1:80 in the sera taken approximately 2 months later. During the same period there was no significant change in CF antibody titer against the RI-APC-ARD virus or in HA1 antibodies for any of 5 strains of influenza virus. Finally, neutralizing antibody against CCA developed in both chimpanzees during the period between bleedings. The etiologic relation between CCA and the epizootic disease in the chimpanzees is supported further by the data obtained when sera of all 20
animals involved in the Forest Glen epizootic were examined for specific complement fixing antibody. As shown in Table II all 14 chimpanzees that experienced clinical coryza during the 3rd week of Oct., 1955, subsequently developed specific antibody. Four other animals that did not suffer clinical coryza likewise produced antibody, hence, they presumably experienced unrecognized infection. The remaining 2 animals apparently escaped infection; they neither suffered clinical disease nor developed CCA CF antibody.
Morris et al. attempted to experimentally recreate inflammation of the mucous membrane by taking toxic unpurified cell culture supernatant said to contain the “virus” and inject it directly into the noses of three monkeys. Two of the three monkeys developed sneezing, coughing, and nasal discharge after the nose goo injections while the third monkey remained unfazed. In another damning blow to their “viral” theory, two of the three control animals also developed disease after having uninoculated toxic cell culture goo injected into their noses. Thus, no “virus” was necessary to recreate the disease, and it could be easily surmised that the injection of toxic soup with or without an imaginary “virus” resulted in nasal discharge.

Experimentally induced coryza in chimpanzees. Three chimpanzees, 20 to 24 months of age and weighing 16 to 20 lbs were inoculated intranasally on Feb. 2, 1956 with 1.0 ml of 11th passage tissue culture material containing 10,000 TC ID50 of CCA. At the same time 3 other chimpanzees housed in the same room were injected intranasally with an uninfected Chang liver cell preparation. Results of this experiment are presented graphically in Fig. 1. Three days (Feb. 5) after inoculation 2 of the 3 chimpanzees receiving CCA developed respiratory illnesses characterized by sneezing, coughing and subsequently mucopurulent nasal discharge. These signs increased somewhat in severity and persisted at this level for 4 to 5 days; however, the animals were not febrile. By the 14th day the affected chimpanzees were free of signs of respiratory disease. The third chimpanzee in this group (Babe in Fig. 1) remained well throughout the period of observation. Of particular interest is the finding that this anlimal possessed CF and neutralizing antibodies (titers 1:40 and 1:20, respectively) at the time of inoculation. Two of 3 control chimpanzees that were housed with animals inoculated with CCA also developed disease. Onset of illness in these control animals occurred on the 7th (Feb. 9) and 9th (Feb. 11) day after receiving the non-infectious cell cultures, or 4 and 6 days, respectively, after the test animals had first exhibited symptoms. None of these chimpanzees developed fever.
Here we see more evidence that even from the control animals subjected to “non-infectious” materials, the same CPE was produced in the cell culture as seen from that observed in samples from “infected” monkeys thus showing no “virus” was necessary to produce the effect.
From each of the 4 chimpanzees that developed obvious respiratory illness, i.e., 2 test and 2 control animals, an agent cytopathogenic for liver cells was recovered from throat swabs taken on Feb. 8. In addition, a cytopathogenic agent was recovered on Feb. 15 from throat materials from the third chimpanzee receiving non-infectious materials. This animal, (Blondy in Fig. 1) did not show recognizable respiratory disease; nevertheless she developed complement fixing and neutralizing antibodies in minimum amounts. Each of the 5 recovered agents was shown to be similar to or identical with CCA in neutralization tests with specific antisera prepared in rabbits against the Sue strain and in complement fixation tests with a human serum that was known to react with CCA antigen.

It may be mentioned here that the 6 chimpanzees in this experiment (Fig. 1) were challenged by the intranasal instillation of 1 ml of tissue culture material containing 1000 TC LD50 of CCA on March 28, 1956, 55 days after the original exposure when each animal possessed demonstrable CF (range 1:20 to 1:160) and neutralizing (range 1:10 to 1:20) antibodies. All 6 chimpanzees remained free of clinical evidence of disease during an observation period of more than a month; moreover, during the same 30 day period there was no appreciable change in serum antibody titers.
Morris et al. tried very hard to claim that a lab worker was infected with “CCA” by way of antibody results as they were unsuccessful in producing the CPE in the culture from the sample taken from this person. Thus, he was presumed to have been infected based upon nonspecific indirect antibody results after the “gold standard” cell culture failed.
Infection of laboratory worker with CCA. During the second week of February 1956, an illness diagnosed clinically as “upper respiratory infection” occurred in a laboratory
worker who was working with CCA and who had had intimate contact with the experimentally infected chimpanzees. His illness was characterized by several days of nasal snuffiness, rhinorrhea, cough, malaise. followed by several days of low grade fever and frontal headache. CF and neutralizing antibodies against CCA were undetectable in the sera of the patient taken on Feb. 8, 1956. but titered 1:80 on Feb. 22, 1956. The single attempt to recover a cytopathogenic agent from throat washings taken on the 6th day of this man’s illness was not successful. The serologic findings which are shown graphically in Fig. 1 (Patient B1) are taken as presumptive evidence that the CCA was of etiologic significance in the patient’s illness.

Serologic reaction of CCA with sera obtained from animals immunized against different viruses. Sera obtained from animals immunized against a variety of viruses were examined in complement fixation and neutralizing tests for their ability to react with CCA. The antisera included those prepared in monkeys against the Enders strain of measles virus* (5) , Chanock’s croup virus* (6) and Sabin’s chimpanzee rhinitis 19 54 virus* (7): in rabbits against several strains of Coxsackie virus, (Group A, type 9 and Group B. types 1, 2, 3 and 4): certain “orphan” viruses (8) [Walter Reed prototypes 7043 (untyped), 7045 (ECHO type 6) and 7054 (ECHO type 2)] and simian virus SV5 (4) and in chickens against simian virus SV59 (4) .) All these anti-sera failled to react with CCA in complement fixation or neutralization tests.
In even more “highly-reliable” antibody testing results, Morris et al. showed that people who were said to have other “viral” infections also possessed the same antibody said to be specific to “CCA.”
Occurrence of antibody against CCA in human sera. Results of CF tests to determine the occurrence of CCA antibody in different age groups in the human population are given in Table III. The sera were obtained from patients at the Walter Reed Army Medical Center with a variety of illnesses. It is evident from the tabular data that a number of human beings possessed CF antibodies that react with CCA antigen. Furthermore, such
antibodies were uncommon in children but were present in about 20% of the persons in the small group of adolescents and young adults examined. It is of some interest that the 40 young adults listed in the table were barrack mates of patient B1. Paired sera from groups of patients with common cold, bronchitis, cold agglutinin positive primary atypical pneumonia, and RI-APC-ARD infection (3 pairs in each category) were tested for complement fixing antibody against CCA. Certain of these tests were performed by Dr. Sidney Katz in Dr. John Dingle’s laboratory in Cleveland using their sera and antigen supplied by us. None of the patients displayed a significant increase in CCA antibody. Nevertheless, certain of the patients possessed throughout their illnesses constant amounts of CCA antibody with titers ranging up to 1:80.
The summary provides a nice overview of how Morris et al. worked hard to convince themselves that they had uncovered a new “virus” from one monkey even though it was not pathogenic to laboratory animals, could only be presumptively associated by way of indirect nonspecific antibody results with a sickened lab worker, and could only be considered a “virus” if all of the contradictory evidence obtained via controls was ignored. Note that they attempted to say that despite being unable to directly link the new “virus” to human disease, the indirect nonspecific antibody results seen in people with unrelated respiratory diseases suggested that they had contact with “CCA” or an unknown related “virus.”
Summary. A virus was recovered from throat materials of a chimpanzee with coryza during an epizootic of (respiratory disease in a colony of these animals. The new agent produced degenerative changes in tissue culture, but was not pathogenic for common laboratory animals. The donor chimpanzee as well as other chimpanzees involved in the epizootic developed specific antibodies against the coryza agent during the months following the outbreak. Susceptible chimpanzees following intranasal instillation of tissue culture materials infected with the coryza agent developed clinical coryza and subsequently made specific antibody. A presumptive etiologic association was established between the new agent and respiratory illness in a laboratory worker, but has not been implicated in the illnesses of small groups of patients with several common types of respiratory disease. However, a number of human beings, particularly adolescents and young adults, have antibodies in their sera directed against the coryza agent suggesting that these individuals have experienced infection with the new agent or one closely related to it.
doi: 10.3181/00379727-92-22538.

In all honesty, the above paper may very well be the worst evidence of a new “virus” that I have ever had the displeasure of reading. The lengths that Morris et al. went to in order to deny the contradictory evidence seen in the controls so that they could convince themselves that they had a new “virus” was impressive. In order to state with a straight face that they had discovered a “virus,” Morris et al. had to:
- Disregard only being able to “isolate” the agent from 1 out of 14 chimpanzees with the same symptoms of disease
- Overlook the fact that the control monkeys used in pathogenicity experiments were older and had already been experimented on for hepatitis “virus” research
- Ignore that the same “viral” inclusion bodies were seen in cultures from both the “infected” and the “uninfected” control monkeys
- Turn a blind eye to the inability to make numerous animals sick through different modes of injection
- Dismiss finding the same “non-viral foamy agents” seen in previous studies using monkey kidney cells which created indistinguishable CPE making interpretation difficult
- Make excuses for why healthy animals showing no signs of illness experienced a rise in antibodies
- Disregard the fact that only 2 out of 3 “infected” animals became sick while 2 out of 3 “uninfected” control animals also became sick
- Dismiss the fact that cytopathogenic “agents” were found in 3 control animals and only in 2 “infected” animals
- Look past the fact that they were unable to isolate a “virus” from a lab worker said to be “infected” and could only presume “infection” based upon nonspecific indirect antibody results
- Rationalize finding the same antibody responses in cases of respiratory disease not said to be caused by their chimpanzee coryza agent
Essentially, Morris et al. completely ignored the contradictory evidence from their control experiments that should have led them to the conclusion that the experimental conditions created the effects observed rather than an imaginary “virus.” Instead, Morris et al. found ways to try and rationalize and explain away the contradictions so that they could claim the successful “isolation” of an invisible “virus” that they never observed directly, nor could they prove indirectly through experimentation. We could end this investigation right here with “RSV,” as every paper afterward was built upon the fraudulent foundation of the unscientific conclusions and evidence drawn from this single paper.
However, my curiosity always gets the better of me. As the 1957 paper by Chanock et al. was also referenced as being essential to the discovery of “RSV” in children, I had to take a look to see what kind of evidence these researchers uncovered a year later which could potentially salvage the train-wreck I had just read. Presented next is the full 1957 paper with commentary.
Recovery from infants with respiratory illness of a virus related to chimpanzee coryza agent (CCA). I. Isolation, properties and characterization
To begin with, Chanock et al. claim that two agents recovered from children with respiratory disease were indistinguishable from Morris et al.’s CCA. As usual, no assumed “viral” particles were ever purified and isolated directly from the fluids of the sick children. Instead, throat swabs from infants with respiratory illness and those with nonrespiratory illness were immediately immersed in 5 ml of Hanks’ solution containing 2,000 units of penicillin, 2,000 micrograms of streptomycin and 150 units of mycostatin per ml. before culturing. These samples were added to unpurified cell cultured creations consisting of either:
- Human epidermoid carcinoma grown in either human or horse serum, washed in Hank’s solution, and maintained in Eagles medium with chicken serum
- Human liver epithelium grown in Eagles medium with 20% horse serum which was also maintained in Eagles medium with 4% horse serum
- Human amnion cultures prepared in Medium 199 with horse serum
- Monkey kidney cultures maintained in Medium 199 with calf serum added for growth
As can be seen, this process is the exact opposite of purifying and isolating any “virus” and consists of creating a toxic mixture of human and animal fluids with synthetic chemicals.
INTRODUCTION
The present study was undertaken in an attempt to recover new cytopathogenic agents from infants with severe lower respiratory illness (bronchopneumonia, bronchiolitis, and laryngotracheo-bronchitis) and to assess their etiologic significance in this disease complex. During the course of these investigations, two similar viruses were recovered -which were demonstrated to be indistinguishable from an agent associated with an outbreak of coryza in chimpanzees (CCA virus) studied by Morris, Blount and Savage (1). It is the purpose of this communication to describe the isolation, properties and characterization of these agents. In the second paper of this series (2) the epidemiologic aspects of human infection with these viruses will be discussed.
MATERIALS AND METHODS
Tissue culture. The KB strain of human epidermoid carcinoma was grown in the chemically defined medium of Eagle (3) containing either 10 percent normal inactivated (56 C) human or horse serum. Prior to use, the cultures were washed 3 times with Hanks’ solution. Maintenance medium consisted of Eagle’s medium with 2 percent inactivated chicken serum. The Chang strain of human liver epithelium (4) was grown in Eagle’s medium with 20 percent inactivated horse serum and maintained in Eagle’s medium with 4 percent inactivated horse serum. Maintenance medium for KB and liver cultures was changed every 3 to 4 days.
Human amnion cultures were prepared according to the method of Takemoto and Lerner (5). Maintenance medium for these cultures consisted of Medium 199 with 4 percent inactivated horse serum. Monkey kidney epithelial cultures were prepared and maintained in Medium 199 (6). For growth, 2 percent inactivated calf serum was added whereas the maintenance medium contained no serum.
Specimens for virus isolation. Throat swabs from infants with respiratory illness and infants with nonrespiratory illness were immersed in 5 ml of Hanks’ solution containing 2,000 units of penicillin, 2,000 micrograms of streptomycin and 150 units of mycostatin per ml. Specimens were tested immediately or after storage at — 50 C. Two tenths ml of throat swab fluid was inoculated into each of 3 to 4 monkey kidney epithelium, KB and human amnion cultures.
Once again, I will be glossing over the indirect nonspecific antibody testing and results for the same reasons, as explained with regards to the previous paper.
Infectivity titrations and neutralization tests in tissue culture. These tests were performed as described previously (7). Twenty to 200 TCD50 of virus as measured by simultaneous titration were employed in the neutralization
tests, which were read on the third or fourth day. Chang liver cultures were used in all neutralization tests.
Complement fixation. The method of Osier, Strauss and Mayer (8) was employed. Briefly, 0.2 ml of serum dilution, 5 C’H|s0 (50 percent hemolytic dose) of complement contained in 0.5 ml, and 0.5 ml of antigen were incubated at 3 to 5 C for 18 hours followed by 20 minutes at 37 C, after which 0.3 ml of sensitized sheep erythrocytes was added and the test incubated at 37 C for 1 hour. Positive serum controls, anticomplementary controls and a complement titration were included in each test.
Complement-fixation (CF) antigens were prepared from infected KB cultures which were frozen and thawed twice and centrifuged at 1,500 rpm for 30 minutes. The supernatant fluid containing the antigen was stored at 50 C.
In this next section, we can see that the size of the “virus” was indirectly estimated as no actual “viral” particles were ever observed.
Measurement of particle size. Virus particle diameter was estimated by a modification of the method of Pardee and Schwerdt (9) which will be described in the text. The swinging bucket rotor (SW 39) of the Spinco Model L ultracentrifuge was used in the present experiments. The titrations for infectivity were performed with 3.2-fold dilutions and 8 culture tubes per dilution. The standard error of these titrations, as calculated by the method of Pizzi (10), was less than 10v0.2.
Chanock et al. used the density and particle diameter of “purified polio” to determine the centrifuge constant. However, there is a slight problem as polio was never purified nor isolated, as explained here, here, and here.
The centrifuge constant (K) was determined experimentally with purified type 1 poliovirus whose density and particle diameter are known. A suspension containing 1,000 PFU (plaque-forming units) per ml was employed. Infectivity titrations were carried out at 3-fold dilutions with four 100- millimeter monkey (Erythrocebus patus) kidney monolayer plates per dilution. The value of K obtained was 3.1 X 10^6.
Look at the ridiculous and inconsistent methods used to create antiserum. Why were the rabbits given more injections than the guinea pigs, and why were there additives such as 2 ml of a mixture of Mycobacterium, butyricum, paraffin oil and arlacel? Also note that the CCA agent was provided to Chanock et al. by Morris et. al as was the case for the antiserum of other “viruses,” which were all provided by different researchers (including Enders) that used their own methods and recipes to create these substances.
Production of antiserum. Guinea pigs were immunized by 3 weekly intraperitoneal inoculations of 1 ml of infected tissue-culture fluid. Rabbits were given 3 weekly intravenous inoculations of 1 ml each followed by 2 weekly intramuscular inoculations of 1 ml of infected culture fluid combined with 2 ml of a mixture of Mycobacterium, butyricum, paraffin oil and arlacel.
Other viruses. The chimpanzee coryza agent (CCA) was kindly provided by Dr. J. A. Morris and Maj. E. Buescher.
Immune sera for other viruses. Specific antiserum for various viruses was kindly supplied by the following investigators: chimpanzee sera for CCA virus by Dr.’J. A. Morris and Maj. E. Buescher; monkey serum for measles by Dr. J. F. Enders, rabbit and chicken serum for mumps by Dr. F. B. Bang; human serum for psittacosis by Dr. A. G. Osier; and rabbit and human serum for primary atypical pneumonia (PAP) virus by Drs. Chien Liu and M. D. Eaton.
RESULTS
Chanock et al. based their “virus” off of 2 instances of CPE observed in 2 out of 59 patients (one with bronchopneumonia and the other with laryngotracheobronchitis) which could only be produced in the KB and liver cultures but not in the monkey kidney or human amnion cultures. The other 57 patients suffering through the exact same symptoms must not have had any “virus” based on these findings. It was noted that serial passaging the culture led to a quicker observation of the CPE. However, serial passaging is known to affect the cell culture as it is disturbed, and the toxic chemicals are refreshed, leading to quicker cell death.
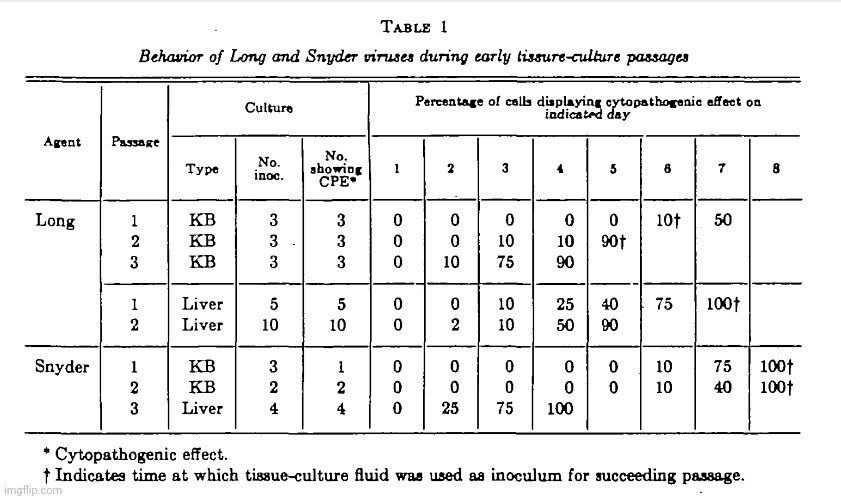
Isolation of agents. An unusual cytopathogenic agent was recovered in KB culture from the throat swab of one of 41 patients with bronchopneumonia (patient Long) and from one of 18 individuals with laryngotracheobronchitis (patient Snyder). Henceforth these agents will be referred to as Long virus and Snyder virus. Attempts to recover these agents after inoculation of throat swab fluid into monkey kidney and human amnion cultures were unsuccessful, although these cultures were held for 3 to 4 weeks in good condition.
The behavior of these agents during their early tissue-culture passages is shown in table 1. The interval before cytopathogenic effects were observed after inoculation of Long virus decreased during the second and third KB passages. The behavior of the virus during the third KB passage was typical of the virus in subsequent passages.
Long virus was reisolated from the original throat swab fluid in cultures of human liver epithelium (Chang strain). It is of interest that the incubation period during the first passage in liver was shorter than that observed in KB culture.
Patient Long developed both CP (a titer of < 1 in 4 in the acute serum and 1 in 80 in the convalescent serum) and neutralizing antibodies (a titer of < 1 in 4 in the acute serum and 1 in 64 in the convalescent serum) for Long virus. Patient Snyder developed CF antibody for Long virus ( a titer of < 1 in 4 in the acute serum and 1 in 8 in the convalescent serum) but tests with the homologous virus could not be performed because of insufficient serum.
Here, we can see the lengths the researchers will go to in order to create the cytopathogenic effect that they want to observe. While Chanock et al. could not culture their “virus” in human amnion cells from the throat swab fluids of sick patients, they claimed that after culturing the “virus” in KB cells that they could get an effect in human amnion cells, albeit after a much longer culturing period and never a complete effect. In other words, they created an unpurified mixture in KB cells and added this to the human amnion culture, which was obviously more toxic to the cells than the original throat swab samples containing less contaminants, and claimed success even though the CPE took much longer to observe and was incomplete.
Cytopathogenic effect in tissue culture. Both Long and Snyder agents produced cytopathogenic effects in liver and KB cultures. With undiluted tissue-culture fluid these effects were observed within 2 to 3 days while minimal quantities of virus required 5 to 8 days. After isolation in KB cultures, Long virus produced an effect in human amnion culture. A longer interval was required in amnion cultures before cytopathogenic changes were observed and progression was very slow. Thus Long KB passage 1, when inoculated into KB cultures, produced an effect within 3 days and almost complete destruction of the cell sheet occurred by the fifth day, whereas amnion cultures inoculated simultaneously with the same material did not show an effect until 9 to 14 days, and the entire cell sheet was not involved by the twenty-second day.
The sensitivity of KB and liver cultures for Long virus was the same. A simultaneous titration of Long KB passage 5 in liver and KB cultures gave the same titer, i.e., 10^5 TCDv50 per ml.
The KB cells, which succumbed to the toxic recipe faster, were shown to have further damage than the liver and amnion cultures by the appearance of round cell degeneration.
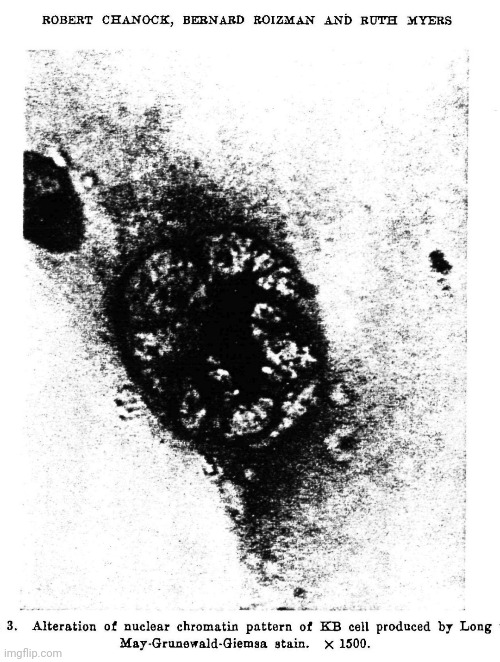
The most striking effect of Long virus in tissue culture was the formation of syncytial areas. In KB cells a round cell degeneration also occurred but syncytium formation predominated. In liver and amnion cultures only syncytial areas were seen. The syncytial areas were characterized by a loss of cell boundaries and the accumulation of a varying number of intact nuclei in a region of homogeneous cytoplasm (figures 1 and 2). The chromatin pattern of the nucleus was altered (figure 3). Thick chromatin strands appeared to radiate peripherally from a thick central mass indistinguishable from an inclusion body. Involved areas of infected liver cultures were similar to those seen in KB cultures.
Cytopathogenic changes were first seen as small circumscribed syncytial areas which were randomly distributed and which enlarged over a 24-hour period, at which time numerous other syncytial areas made their appearance. Usually, within 1 to 4 days the entire cell sheet was involved.
As no “viral” particles were ever observed, Chanock et al. utilized indirect means to estimate the size of the invisible particles. They extrapolated (the action of estimating or concluding something by assuming that existing trends will continue or a current method will remain applicable) from centrifugation in sucrose solutions. The researchers admitted that the method they used was a crude estimate and needed confirmation by more refined measures. Perhaps having the actual “viral” particles visually on hand would help?
Physical properties. The diameter of Long virus was determined by centrifugation in sucrose solutions of varying concentrations by a modification of the method of Pardee and Schwerdt (9). Supernatant fluids were titrated for the residual infectivity. When the percentage of unsedimented virus was plotted against sucrose density the sucrose density at which all virus was sedimented was obtained by extrapolation. The sucrose density at which no virus was sedimented was also obtained by extrapolation. The viscosity corresponding to the extrapolated sucrose density values was calculated from the data given by Bates (11). From these values the particle diameter was derived by the formula given in table 2. In two independent experiments particle diameters of 105 and 107 millimicrons were obtained. The corresponding hydrated particle density values were 1.19 and 1.26. If these density values are taken as a range then the particle diameter may be estimated to be within a range of 90 to 130 millimicrons. It should be noted that the method employed for the determination of size merely provides a rough estimate that will require confirmation by more refined methods.

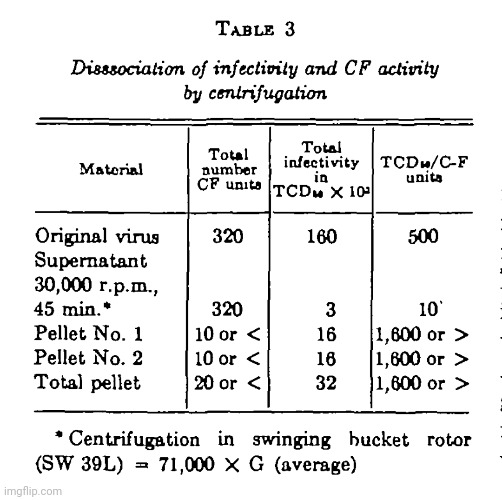
The antigen responsible for complement fixation appears to have a smaller sedimentation constant than the infectious particle. Thus, centrifugation at 30,000 r. p. m. for 2.5 hours in the number 30 rotor of the Model L Spinco ultracentrifuge (78,410 X G average) failed to diminish the CF antigen titer of the supernatant fluid. Following additional centrifugation at 40,000 r.p.m. for 3 hours in the number 40 rotor (105,000 X G average) the potency of CF antigen in the supernatant fluid remained unchanged.
It was possible to dissociate infectivity and CF antigen activity by centrifugation as shown in table 3. CF antigen was quantitatively recovered from the supernatant fluid while the pellets contained 90 percent of the recoverable infective virus without any detectable CF antigen.
In this section, Chanock et al. tried every which way to get their “virus” to infect chickens or multiply in embryonated eggs but were unsuccessful at every attempt. They could also not get their “virus” to sicken one-day-old mice by way of injection into the brain or into the space between the muscles and organs in the abdomen.
Other properties. Exposure of Long virus to 20 percent ether for 16 hours at 4 C resulted in complete loss of infectivity. Attempts to demonstrate a hemagglutinin for chicken or human “O” erthrocytes were unsuccessful. No pocks were seen 3 days after inoculation of 10 and 100 TCDv50. of Long virus onto the chorioallantoic membrane of the 11-day embryonated egg. Multiplication of Long virus could not be demonstrated when 9-day embryonated eggs were inoculated with 10,000 TCD50 into the amniotic sac and incubated for 6 days. Long virus was not pathogenic for 1-day-old mice by the intracerebral or intraperitoneal route. Long virus could be filtered through gradocol membranes of 590 and 960 millimicrons average pore diameter.

Chanock et al. attempted to connect the Long and Snyder “virus” to Morris et al.’s CCA by way of the pattern of CPE observed in liver and KB cultures as well as indirect nonspecific antibody results. Note that neither the CCA nor the Long/Snyder “viruses” had ever been observed in order to be characterized nor compared. The researchers also used these same indirect means, mostly relying on antibody results, to claim that their “virus” was unrelated to other “viruses.”
Relationship to CCA virus. CCA virus was received in the laboratory after
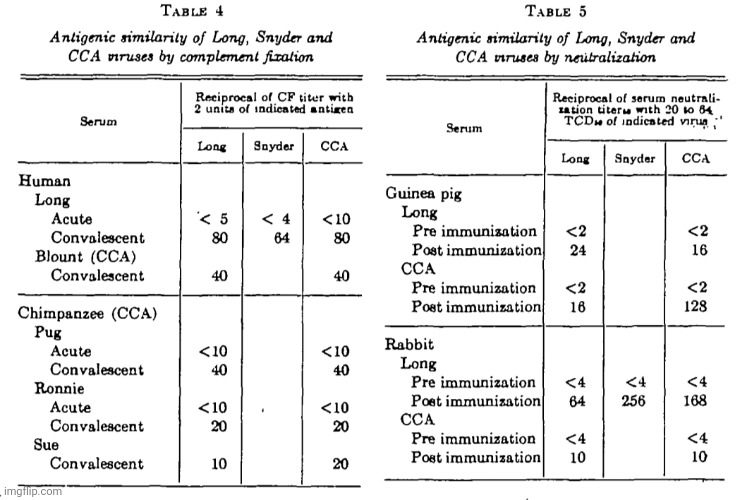
Long virus had been isolated. CCA virus produced a cytopathogenic effect in liver and KB cultures which was identical to that seen with Long and Snyder viruses. By CF tests with paired human and chimpanzee sera (table 4) Long and Snyder viruses were indistinguishable from CCA virus. In neutralization tests with sera from immune guinea pigs and rabbits (table 5). Long, Snyder and CCA viruses reacted in a similar manner except for the tests with CCA immune guinea-pig serum. Although the postimmunization CCA guinea-pig serum neutralized Long virus, the homologous titer with CCA virus was 8-fold higher.
Relationship to other viruses. The cytopathogenic effects produced by Long virus was distinct from that characteristic of the adenovirus group. Long virus was not related antigenically to the adenoviruses as shown by the nonassociation of rises in CF antibody for Long and adenoviruses in infants with
or without respiratory illness (table 6). The history of these infants will be described more completely in the accompanying communication (2).
Long virus was not antigenically related to other human viruses which produce syncytial changes in tissue culture (table 7).

Long virus was distinct from the primary atypical pneumonia (PAP) virus of Liu and Eaton (12). A 1-in-4 dilution of a serum from a PAP immune rabbit (homologous titer of 1 in 256) failed to neutralize Long virus. In addition, CF antibody for Long virus was not detected nor was a change in Long neutralizing antibody observed with paired serum specimens from a PAP patient who developed neutralizing antibody for PAP virus during convalescence.

Long vims was not related to the psittacosis-LGV group of viruses since a human serum with a psittacosis CF titer of 1 in 160 failed to fix complement in a l-in-5 dilution with Long CF antigen.
DISCUSSION
In the discussion section, we get the statement that the CPE and antigenic properties between Long/Snyder and CCA were similar (not identical as previously stated) and yet they claim their agents were indistinguishable from each other. However, a pretty revealing statement was made where Chanock et al. admit that their findings did not prove that Long and Snyder “viruses” were responsible for the associated illnesses in infants. Enough said.
Morris, Blount and Savage recovered a virus (CCA) from an outbreak of mild respiratory illness in chimpanzees (1). This illness, was reproduced in susceptible chimpanzees by the intranasal instillation of tissue-culture CCA virus. In the present study two viruses (Long and Snyder), which were similar in tissue-culture cytopathogenic effect and antigenic properties with CCA virus, were recovered from infants with severe lower respiratory illness. The development of antibody to Long virus during the convalescence of these infants confirmed that Long and Snyder viruses were derived from human sources. It is clear, therefore, that agents indistinguishable from CCA virus are capable of causing human infection. However, this does not prove that Long and Snyder viruses were responsible for the associated illnesses in these infants. This problem and the role of this group of agents in respiratory illness of infancy will be considered in the accompanying communication (2).
The most striking property of Long and Snyder viruses was their ability to produce large syncytial areas in KB and liver cultures. Of the viruses which infect human beings only measles, mumps and CA viruses have been previously shown to produce syncytial changes in cultures of various types (7, 13, 14). Antigenically these viruses are distinct from the agents isolated in this study. In addition, mumps and CA viruses can be distinguished by their ability to agglutinate human and chicken erythrocytes. Measles virus produces syncytial changes in KB cultures but at least 5 weeks are required for complete cell destruction (15) whereas Long and Snyder viruses destroy the cell sheet within 3 to 6 days.
Similar to the adenoviruses, Long virus produces a CF antigen distinct from the infectious particle. However, the type of cytopathogenic effect produced in KB cultures, ether sensitivity and the lack of antigenic relationship in CF tests with human sera clearly distinguish Long virus from the adenovirus group.
SUMMARY
Two viruses, which were indistinguishable from an agent associated with coryza in chimpanzees (CCA virus), were recovered from infants with lower respiratory illness. The agents isolated in this study were characterized by the occurrence of a syncytial cytopathogenic effect in KB or human liver tissue culture and the production of a CF antigen which was separable from the infectious particle by centrifugation. The particle diameter was estimated to be 90 to 130 millimicrons. These agents were not related to the adenovirus group nor to other currently known viruses which cause respiratory illness.
https://doi.org/10.1093/oxfordjournals.aje.a119901

What we got from Chanock et al.’s first paper from 1957 was the usual cell culture concoction that was apparently very difficult to create. It took many cell lines and various tricks by the researchers to try and get the preconceived cytopathogenic effect that they wanted to see. Even then, the researchers were largely unsuccessful with their attempts and had to rely on indirect nonspecific antibody results to try and claim the “virus” was present and that it was somehow related to the CCA “virus” that Morris et al. “discovered” in chimpanzees the year prior. It is therefore understandable, given the incredibly flimsy evidence obtained, why Chanock et al. stated their evidence did not prove that Long and Snyder “viruses” were responsible for the associated illnesses in infants. Thus, they left it to a second paper to provide this evidence for them. Ironically, it did no such thing.
With Chanock et al.’s second paper from 1957, you will see that the “proof” that was promised was just as poor, if not more so, than that presented within the first paper. I provided commentary and highlights for the pertinent information but edited out much of the invalid antibody results. If you desire to see the researchers’ attempt to use one hypothetical entity to try and prove another, please feel free to download the linked paper.
Recovery from infants with respiratory illness of a virus related to chimpanzee coryza agent (CCA). II. Epidemiologic aspects of infection in infants and young children
In the introduction, Chanock et al. attempt to make a case that Morris et al. had discovered a “virus” in captive chimps by “finding” evidence of a “virus” in 1 out of 14 chimpanzees. However, they were unable to “isolate” the same “virus” from a sickened lab worker. Fortunately, the researchers were able to use indirect nonspecific antibody results to claim that the invisible “virus” truly was present even though it could not be found nor observed.
INTRODUCTION
“Morris, Blount and Savage (1) studied an outbreak of coryza in a colony of chimpanzees held under observation for 3 to 24 weeks prior to the onset of illness. A virus (CCA) was recovered from one of the 14 affected chimpanzees and the remaining 13 animals developed antibody to this virus during convalescence. A person working with the infected chimpanzees subsequently experienced a respiratory infection and, although virus isolation attempts were unsuccessful, a rise in antibody for CCA virus was observed during convalescence. When susceptible chimpanzees were inoculated intranasally with tissue-culture CCA virus, coryza was observed after a 3-day incubation period. These findings suggested the possibility that CCA was a virus of human origin which produced an outbreak of mild respiratory illness when introduced into a susceptible population of chimpanzees.
Of their own findings, Chanock et al. stated that antibody results from children where “viruses” were recovered led them to believe that their invisible “viruses” were indistinguishable from Morris et al.’s CCA chimpanzee “virus.” However, they admitted that the results could not be interpreted to mean that these “agents” were the cause of the illnesses in the infants.
During a study of infants with lower respiratory disease (2) two agents (Long and Snyder) were recovered which were indistinguishable from CCA virus. The infants from whom the viruses were recovered developed antibody during convalescence. From these findings it is clear that viruses which are indistinguishable from CCA virus are capable of infecting human beings. These results cannot be interpreted to mean that these agents were the cause of the illnesses in the infants, since the temporal association of disease and infection with an agent is only the first step in the chain of evidence required for etiologic significance (3).
Oddly enough, only infants considered to have severe lower respiratory disease were studied. Children with mild respiratory disease were not studied as these symptoms were said to be common and more difficult to diagnose accurately.
This communication will describe preliminary investigations which were designed to provide an understanding of the epidemiology and pathogenicity for infants of the CCA-Long-Snyder group of agents. Infants with severe lower respiratory illness and a control group of infants without such illness were studied. Mild respiratory illnesses were not studied because of the frequency with which these illnesses occur during the winter months in this age group (4), and since clinical diagnosis is less accurate than in infants with severe illness.

MATERIALS AND METHODS
In the methods section, it can be seen that the children studied were those with severe lower respiratory illness and that controls consisted of infants and children without respiratory illness. The children with respiratory illness were diagnosed with non-bacterial pneumonia as their illness was said not to resemble bacterial infection, even though both bacterial and “viral” pneumonia have the same clinical picture. The controls differed from the respiratory illness cases in that the proportion of hospitalized individuals was smaller and were, on average, older than the patients with respiratory illness.
Study population. The study population consisted of infants and children under 4 years of age with severe lower respiratory illness and a control group of infants and small children who did not have respiratory illness at the time specimens for virus isolation were obtained. The subjects were from a low socioeconomic environment.
Infants and small children up to the age of 4 years who were admitted to either the Harriet Lane Home of the Johns Hopkins Hospital, Baltimore, Md., or the Pediatric Division of the Baltimore City Hospitals with the diagnosis of bronchopneumonia or bronchiolitis constituted the hospital respiratory group. Patients up to 4 years of age with bronchopneumonia who were seen in the outpatient clinic of the same institutions constituted the outpatient respiratory group. Bronchopneumonia was diagnosed when tachypnea, fine moist rales and, in most instances, pulmonary infiltration occurred. The clinical course of the patients selected for this study did not resemble that of a bacterial pneumonia. Chest x-rays were taken on all ward patients with pneumonia and on the majority of the outpatients with pneumonia. Bronchiolitis was diagnosed when tachypnea, expiratory wheezing, prolongation of expiration, and evidence of emphysema were observed. In addition, it was not uncommon for moist rales and x-ray evidence of pulmonary infiltration to occur in infants with bronchiolitis.
The controls were children with non-respiratory illnesses from the outpatient clinics of the Harriet Lane Home and Baltimore City Hospitals and from the pediatric ward of the latter hospital. Patients with infectious disease were not admitted to this ward.
The study extended from October, 1956, to March, 1957. The respiratory patients and the controls were distributed over this 6-month intervaL
The same procedure was employed in studying the various groups. A throat swab and a blood specimen were obtained at the time of admission to the hospital or during the first clinic visit. An attempt was made to obtain a second serum sample 4 weeks later. In many instances a second sample could not be secured until after an interval of 6 to 10 weeks, and in several instances 12 weeks.
Table 1 shows the number of children in each group, their average age in months and the mean intervals between serum samples. It will be seen that the controls differed from the respiratory illness cases in that the proportion of hospitalized individuals was smaller. The controls were, on the average, older than the patients with respiratory illness.
Laboratory procedures. The techniques for virus isolation, complement-fixation (CF) and neutralization tests in tissue culture have been described (2).”

Amazingly, we find out that the Long “virus” was only able to be “isolated” from one infant with bronchopneumonia. Attempts to “isolate” the “virus” from 12 infants with bronchopneumonia, 28 infants with pneumonia, and 90 infants with bronchiolitis were all unsuccessful. They were also unable to “isolate” the “virus” from 151 controls. When attempting liver epithelium cultures for the respiratory patients and controls who showed an antibody response, all results were negative except for the one infant that the “virus” was recovered from. The incidence of “infection” with the “virus” as identified by CP and neutralization tests were not significantly different from the control group. This should show that the antibody results are entirely meaningless.
“Relation of Long virus to pneumonia and bronchiolitis of infancy. Long virus was isolated once in KB tissue culture from the throat swab fluid of a clinic infant with bronchopneumonia. Twelve other isolation attempts with throat swabs from clinic infants and children with bronchopneumonia were unsuccessful as were isolation attempts with specimens from 28 infants with pneumonia and 90 infants with bronchiolitis who were hospitalized. Long virus was not isolated from the throat swabs of 151 control individuals. The throat swabs of respiratory patients and controls who developed a rise in antibody to Long virus were tested in liver epithelium cultures with negative results except for the one patient from whom virus was isolated in KB culture.
In the group of infants hospitalized with pneumonia or bronchiolitis the incidence of infection with Long virus as determined by CP (table 6) or the neutralization technique was not significantly different from that of the control group. The control group was not completely satisfactory in that the average age was considerably older than the average for either respiratory group (table 1). However, the control infants whose age matched that of the respiratory patients exhibited the same incidence of CF antibody development (3 of 12 (25 percent)) as the older controls (4 of 17 (24 percent)). It is possible that some of the respiratory illnesses which required hospitalization were associated with Long virus but this would be difficult to establish because of the high rate of infection in the control group.
The incidence of Long virus infection among outpatients with bronchopneumonia and among outpatient controls is shown in table 7. The mean age and mean interval between serum samples were similar in both groups (table 1).
While Chanock et al. attempted to make a link between their “virus” and bronchopneumonia by way of indirect nonspecific antibody results, they admitted that the small sample size meant that the conclusion could only be tentative and that any association between the two awaited future studies.
It is important to note that the 13 individuals with bronchopneumonia were distributed over the 6-month period of the study and that cases of bronchopneumonia with an antibody rise for Long virus occurred during each of the months except December. The significantly higher rate of infection among the outpatients with bronchopneumonia suggests that an etiologic association exists between Long virus and a certain segment of the bronchopneumonia syndrome. However, since the number of outpatients with bronchopneumonia was small (13 individuals), any conclusions derived from this study must be regarded as tentative in nature. The firm establishment of an etiologic association between Long virus and bronchopneumonia must await future studies.
Detailed information on the 13 clinic patients with bronchopneumonia is
given in table 8. The isolation of pneumococcus or B hemolytic streptococcus from 3 of the 10 nose and throat cultures does not constitute an unusually high proportion of positive findings during the winter months as judged by the results presented by Babe (5). The clinical course of the 3 patients from whom bacterial pathogens were recovered was similar to that of the other patients with pneumonia and did not resemble a bacterial illness.
DISCUSSION
In the discussion, we can see how they try to utilize non-specific antibody reactions to indirectly claim the presence and relation of different “viruses.” In this case, 41 infants with disease and 16 control infants without disease had some form of antibody response. Even though they could not “isolate” the “virus,” it was claimed that these antibody results showed that “infections” were frequent. They compared their inability to “isolate” a “virus” with that of Morris et al. as if this somehow meant that both teams of researchers were successful in identifying the same “virus” even though neither team could “grow” the “virus” regularly. Interestingly, Chanock et al. admitted that CF antibody responses were assumed to indicate and measure infection and then tried to come up with various explanations for why their antibody results did not reflect their expectations. It was stated that it was not possible to determine which of the alternatives they dreamt up offered the correct explanation.
The isolation from infants with lower respiratory disease of two viruses which were indistinguishable from CCA virus indicated that agents of this group are capable of infecting human beings (2). Additional support for this conclusion was the finding that 41 infants with lower respiratory illness and 16 control infants without respiratory disease developed CF antibody, neutralizing antibody, or both, to Long virus during the course of this study.
The frequent occurrence of infection when compared with the infrequent isolation of virus suggests that Long virus is recoverable from the throat during a very short interval following infection. However, it is probable that many of the infections diagnosed by serologic methods in this study occurred after the throat swab was obtained and during the interval between the collection of serum samples. Morris, Blount and Savage (1) experienced similar difficulty in isolating CCA virus from chimpanzees with respiratory illness. In the epizootic of coryza studied by these investigators virus was recovered from only one of 14 affected chimpanzees 4 days after the first respiratory signs were noted.
Acquisition of neutralizing antibody to Long virus occurred very early in life and at a rapid rate. In the present study population, 77 percent of children 3 years of age and 80 percent of children 4 years of age possessed neutralizing activity in their serum. From these findings one would anticipate that infection of older individuals would occur infrequently. However, Morris, Blount and Savage (1) reported that 24 percent of individuals in the age group 10 to 18 years possessed CF antibody for CCA virus. We have observed a similar incidence of CF antibody for Long virus in a group of 67 prisoners (21 through 29 years old) from a Federal prison in Ohio.
Assuming that CF antibody is a measure of recent or persisting infection the findings just described could result from: (a) the occurrence of reinfection during the second and third decade at a time when neutralizing antibody levels have decreased below a certain critical level, (5) the occurrence of persisting infection in a certain proportion of individuals, (c) differences in the make-up of the various study populations, or (d) the occurrence of antigenically related but distinct agents which share a common CF antigen with Long virus. At the present time it is not possible to determine which of these alternatives offers the correct explanation.”
In this next section, we get a pretty glaring admission from Chanock et al. as it is admitted that they could not demonstrate an association between their “virus” and lower respiratory disease in infants. Today, “RSV” is considered the leading cause of lower respiratory disease in infants, so it is quite telling that they could not demonstrate a relationship. The researchers theorized that they could not make a link due to the high rate of “infection” in the control group. It was also admitted that they could make no definitive statement on the pathogenic spectrum of the “virus” in man. All they could say was that from their study, in the majority of infants, “infection” resulted in either mild illness or no discernible disease. All the researchers could state was that they suspected an association with lower respiratory disease in infants.
“An association between Long virus and lower respiratory disease in hospitalized infants was not demonstrable. Possibly, however, such an association does exist but was overshadowed by the high rate of infection among the hospital control group. The lower rate of infection among the clinic controls was considerably less than that for outpatients with bronchopneumonia. Although this observed difference appears to be significant, the number of clinic bronchopneumonia patients was sufficiently small (13 individuals) that the conclusions derived from the data must be considered as tentative.
At the present time a definite statement cannot be made regarding the spectrum of pathogenicity of Long virus for man. It is possible to state that this virus was prevalent among young children in this community during the study period and that in the majority of infants infection resulted in either mild illness or no discernible disease.
Since (a) CCA virus has been shown to produce mild upper respiratory illness in chimpanzees, (b) Long and Snyder viruses were recovered from the throat of infants with lower respiratory illness, (c) Long and Snyder viruses are indistinguishable from CCA virus, (d) Long virus is suspected of an association with bronchopneumonia in infancy, and (e) the striking characteristic of these viruses is the production of syncytial areas in tissue culture, it is suggested that these agents be grouped together and named “respiratory syncytial” (RS) virus until their epidemiology and pathogenicity are better understood.
SUMMARY
In the summary, Chanock et al. wanted to remind us that their flimsy case rested on evidence that was based upon the “recovery” of a “virus” from one infant with bronchopneumonia and that an association of Long “virus” with severe lower respiratory illness in hospitalized patients could not be demonstrated. In other words, they had nothing.
A study was carried out to elucidate the epidemiology of an agent (Long virus) which was recovered from an infant with bronchopneumonia and shown to be indistinguishable from chimpanzee coryza agent (CCA). The neutralization test was found to be twice as sensitive as the complement-fixation technique in the serologic diagnosis of infection in infants and small children. In the present study population, 80 percent of children 4 years of age possessed neutralizing activity for Long virus in their serum. Seven percent of nonhospitalized control infants and children, without overt respiratory illness at the time of initial bleeding, developed antibody for Long virus during an average interval of 6 weeks in the winter months. The rate of infection among a similar control group who were hospitalized on a ward which did not admit patients with infectious disease was 6 times greater than among the outpatient controls from the same hospital.
An association of Long virus with severe lower respiratory illness in hospitalized patients could not be demonstrated, possibly because of the high rate of infection occurring in the ward control group. The data suggested an association between Long virus and bronchopneumonia occurring in outpatients. However, the number of out-patients with bronchopneumonia was small (13 individuals) and thus the conclusions derived from these data must be considered tentative.
It is proposed that the agents isolated in this study and the CCA virus be grouped together and named “respiratory syncytial” (RS) virus.”
https://pubmed.ncbi.nlm.nih.gov/13478579/

In Summary:
- “RSV,” “Covid,” and the “flu” have symptoms that are similar, which can make them difficult to tell apart
- The three “viruses” are said to be more similar to each other than they are different in terms of symptoms
- The absence of one of the symptoms does not mean a patient doesn’t have a particular “virus” and the only way to be sure is to get tested
- If anybody has generic symptoms, such as fever, cough, runny nose, there’s no real way to distinguish which one is which without a test
- The CDC confirmed that clinical symptoms of “RSV” are nonspecific and can overlap with other “viral” respiratory infections, as well as some bacterial infections
- “RSV” was discovered in 1956 but was not initially associated with respiratory illness among infants
- Morris and co-workers “isolated” a new “virus” from chimpanzees originally named chimpanzee coryza agent (CCA)
- Subsequently, Chanock and co-workers “confirmed” that the agent caused respiratory illness in humans when they obtained “isolates” from two children

- Morris et al. stated that the paper described the “isolation” of a “virus” of apparent etiologic significance (seeming to be real or true, but not necessarily so) in the epizootic
- They felt that they had established an etiologic association between the chimpanzee coryza agent and respiratory illness in a single laboratory worker
- Morris presented serologic data suggesting that a number of human beings experienced infection with the chimpanzee coryza “virus” or an agent closely related to it (there goes any claim of specificity)
- Throat swabs from 14 of 20 young monkeys with coryza (inflammation of mucous membrane) provided the material employed for “viral isolation” studies
- Another group of somewhat older chimpanzees was used in studying experimental transmissibility of the coryza and the 6 animals in this group had been inoculated previously with material presumed to contain the “virus” of human infectious hepatitis (thus invalidating them as a valid control)
- Tissue cultures of epithelial-like cells derived from human liver were grown in roller tubes in nutrient medium consisting of 8 parts Eagle’s basal medium, 2 parts inactivated
horse serum, and 0.2 part L-glutamine along with Penicillin (100 uniits/ml) and streptomycin (20 ug/ml) which were added to control adventitious bacterial contaminants - A throat swab from one chimpanzee (Sue) involved in the epizootic was washed in 2 ml of tissue culture nutrient fluid
containing antibiotics - After 4 days incubation the original cell nutrient was replaced with fresh nutrient/antibiotics
- 4 days later, the cytopathogenic effect was observed as the cell died and a “virus” was claimed to be “isolated”
- Similar “isolation” attempts, which were made with
materials obtained from 13 other ill chimpanzees, gave negative results (i.e. they could only “isolate” the “virus” from 1 of the 14 monkeys) - CPE was observed from the one cultured sample after 8 days and inclusion-like bodies (i.e. aggregates of “virus” particles or “virus-induced” proteins or special structures characteristic of infection by “viruses” either in the cytoplasm or the nucleus) were seen in the inoculated culture
- However, similar inclusion-like bodies were demonstrated in uninoculated cells, grown in inactivated horse serum
- The researchers did not know the significance of the inclusion-like structures found in infected and uninfected cells and that nothing could be stated with certainty
- In other words, they found the exact same “viral” structures in the uninoculated control cultures as observed in the one inoculated culture thus proving this effect was not dependent on the presence of an imaginary “virus”
- With the exception of a single guinea pig that developed persistent fever beginning on the 3rd day, none of the inoculated animals or embryonated eggs other than chimpanzees developed signs of disease during observation periods ranging up to 28 days
- The etiology of fever in the guinea pig was ultimately traced to a bacterial infection
- Monkey kidney cells underwent complete degeneration 8 days after infection with CCA but the cytopathogenic effect obtained was difficult to interpret because of the presence in the cultures of adventitious simian “viruses”
- CCA was found to be related to the epizootic disease of chimpanzees at the Forest Glen Annex of the WRAIR by the use of serologic techniques
- Four other animals that did not suffer clinical coryza likewise produced antibody, hence, they presumably experienced unrecognized infection
- The remaining 2 animals apparently escaped infection; they neither suffered clinical disease nor developed CCA CF antibody
- Three monkeys were inoculated intranasally with the “virus” soup and three days later, 2 of the 3 chimpanzees receiving CCA developed respiratory illnesses characterized by sneezing, coughing and subsequently mucopurulent nasal discharge
- Two of 3 control chimpanzees that were housed with
animals inoculated with CCA also developed disease after receiving the non-infectious cell cultures - In other words, no “virus” was necessary to experimentally recreate respiratory disease using either “infectious’ or “non-infectious” toxic cell culture soup injected directly into the nasal cavities of monkeys
- From each of the 4 chimpanzees that developed obvious respiratory illness, i.e., 2 test and 2 control animals, an “agent” cytopathogenic for liver cells was recovered from throat swabs taken on Feb. 8
- In addition, a cytopathogenic agent was recovered on Feb. 15 from throat materials from the third chimpanzee receiving non-infectious materials
- Thus, the same CPE was observed in the cell cultures prepared from the 3 “non-infected” control animals as observed in the 2 “infected” animals which once again demonstrates that no “virus” is necessary to produce this effect
- The single attempt to recover a cytopathogenic “agent” from throat washings of a lab worker who experienced respiratory symptoms was not successful
- Thus, indirect nonspecific serologic findings were taken as presumptive evidence that the CCA was of etiologic significance in the patient’s illness
- Paired sera from groups of patients with common cold, bronchitis, cold agglutinin positive primary atypical pneumonia, and RI-APC-ARD infection (3 pairs in each category) were tested for complement fixing antibody against CCA
- None of the patients displayed a significant increase in CCA antibody yet certain patients possessed throughout their illnesses constant amounts of CCA antibody with titers ranging up to 1:80
- In other words, the antibodies claimed to be specific to “CCA” were found in patients not said to be suffering from “CCA”
- During the course of the investigations by Chanock et al., two similar “viruses” were recovered which they claimed were demonstrated to be indistinguishable from an agent associated with an outbreak of coryza in chimpanzees (CCA)
- The KB strain of human epidermoid carcinoma was grown in the chemically defined medium of Eagle containing either 10 percent normal inactivated human or horse serum
- Prior to use, the cultures were washed 3 times with Hanks’ solution and maintained in medium consisting of Eagle’s medium with 2 percent inactivated chicken serum
- The Chang strain of human liver epithelium was grown in Eagle’s medium with 20 percent inactivated horse serum and maintained in Eagle’s medium with 4 percent inactivated horse serum
- Maintenance medium for KB and liver cultures was changed every 3 to 4 days
- Human amnion cultures were prepared according to the method of Takemoto and Lerner with maintenance medium for these cultures consisting of Medium 199 with 4 percent inactivated horse serum
- Monkey kidney epithelial
cultures were prepared and maintained in Medium 199 while 2 percent inactivated calf serum was added for growth - Throat swabs from infants with respiratory illness and infants with nonrespiratory illness were immersed in 5 ml of Hanks’ solution containing 2,000 units of penicillin, 2,000 micrograms of streptomycin and 150 units of mycostatin per ml
- “Virus” particle diameter was estimated by a modification of the method of Pardee and Schwerdt (as they never observed any “viral” particles)
- The centrifuge constant (K) was determined experimentally with “purified” type 1 “poliovirus” whose density and particle diameter were said to be known (that’s odd as “polio” was never purified nor isolated….)
- To create antiserum, guinea pigs
were immunized by 3 weekly intraperitoneal inoculations of 1 ml of infected tissue-culture fluid while rabbits were given 3 weekly intravenous inoculations of 1 ml each followed by 2 weekly intramuscular inoculations of 1 ml of infected culture fluid combined with 2 ml of a mixture of Mycobacterium, butyricum, paraffin oil and arlacel - An unusual cytopathogenic “agent” was recovered in KB culture from the throat swab of one of 41 patients with bronchopneumonia (patient Long) and from one of 18 individuals with laryngotracheobronchitis (patient Snyder)
- Attempts to recover these agents after inoculation of throat swab fluid into monkey kidney and human amnion cultures were unsuccessful
- In other words, they could only find the “virus” in 2 out of 59 patients suffering from the same symptoms of disease and they could only culture it in KB and liver cultures but not in monkey kidney nor human amnion cultures
- The interval before cytopathogenic effects were observed after inoculation of Long “virus” decreased during the second and third KB passages (not surprising as serial passaging speeds up cell death as the culture is disturbed and the toxic chemicals are refreshed)
- CPE could only be observed in human amnion cultures after the addition of the Long “virus” which was “isolated” in KB cultures first, albeit much more slowly and incomplete
- In KB cells a round
cell degeneration occurred that was not observed in liver and amnion cultures - Cytopathogenic changes were first seen as small circumscribed syncytial areas which were randomly distributed and which enlarged over a 24-hour period, at which time numerous other syncytial areas made their appearance (hence the name of the “virus”)
- The size of the particles was extrapolated (i.e. the action of estimating or concluding something by assuming that existing trends will continue or a current method will remain applicable) using centrifugation and sucrose gradient solutions without any visual evidence of the particles they were supposed to be measuring
- Chanock et al. stated that it should be noted that the method employed for the determination of size merely provided a rough estimate that required confirmation by more refined methods
- Attempts to demonstrate a
hemagglutinin for chicken or human “O” erthrocytes were unsuccessful - Multiplication of Long “virus” could not be demonstrated when 9-day embryonated eggs were inoculated with 10,000 TCD50 into the amniotic sac and incubated for 6 days
- The Long “virus” was also not pathogenic for 1-day-old mice by the intracerebral or intraperitoneal route
- Chanock et al. attempted to make the case that the Long/Snyder “virus” was the same as Morris et al.’s CCA by way of indirect CPE patterns and antibody results and relied mostly on unreliable antibody results to claim that they were unrelated to other “viruses”
- In the discussion, Chanock et al. changed their description of the CPE and antigenic properties observed between their “virus” and CCA as similar rather than the previous descriptor of identical
- While they then claimed that agents were indistinguishable from CCA “virus” and were capable of causing human infection, it was admitted that this did not prove that Long and Snyder “viruses” were responsible for the associated illnesses in these infants
- Of the “viruses” which infect human beings only “measles,” “mumps” and “CA viruses” were previously shown to produce syncytial changes in cultures of various types thus showing that this effect is not specific to “RSV” and the only difference between the “viruses” is unreliable serological results

- Chanock et al. claimed that Morris et al. recovered a “virus” (CCA) from one of the 14 affected chimpanzees
- They stated that the “virus” was linked to a sickened lab worker even though “virus” isolation attempts were unsuccessful
- It was stated that these findings suggested the possibility that CCA was a “virus” of human origin which produced an outbreak of mild respiratory illness when introduced into a susceptible population of chimpanzees
- Only infants with severe lower respiratory illness and a control group of infants without such illness were studied as mild respiratory illnesses were disregarded because of the frequency with which these illnesses occur during the winter months in this age group, and since clinical diagnosis is less accurate than in infants with severe illness
- Keep in mind that the researchers were studying lower respiratory illness with their newly discovered “virus” as this will be important later
- The controls differed from the respiratory illness cases in that the proportion of hospitalized individuals was smaller and were, on average, older than the patients with respiratory illness
- Long “virus” was “isolated” once in KB tissue culture from the throat swab fluid of a clinic infant with bronchopneumonia
- However, twelve other “isolation” attempts with throat swabs from clinic infants and children with bronchopneumonia were unsuccessful as were “isolation“ attempts with specimens from 28 infants with pneumonia and 90 infants with bronchiolitis who were hospitalized
- The throat swabs of respiratory patients and controls who developed a rise in antibody to Long “virus” were tested in liver epithelium cultures with negative results except for the one patient from whom “virus” was “isolated” in KB culture
- Incidence of “infection” with Long “virus” as determined by CP or the neutralization technique was not significantly different from that of the control group
- The researchers felt that it was possible that some of the respiratory illnesses which required hospitalization were associated with Long “virus” but this was difficult to establish because of the high rate of infection in the control group
- They felt that significantly higher rate of infection among the outpatients with bronchopneumonia suggested that an etiologic association existed between Long “virus” and a certain segment of the bronchopneumonia syndrome
- However, it was admitted that since the number of outpatients with bronchopneumonia was small (13 individuals), any conclusions derived from this study must be regarded as tentative in nature
- The firm establishment of an etiologic association between Long “virus” and bronchopneumonia required future studies
- Pneumococcus or B hemolytic streptococcus was isolated from 3 of the 10 nose and throat cultures
- The clinical course of the 3 patients from whom bacterial pathogens were recovered was similar to that of the other patients with pneumonia and did not resemble a bacterial illness
- What exactly the difference was between a bacterial pneumonia and a “viral” pneumonia was not defined and probably for good reason as it is stated that distinguishing between “viral” and bacterial cases can be challenging as both share similar symptoms and biomarkers.
- The researchers attempted to claim antibody results showed the presence and relation of their “virus” with CCA when 41 infants with lower respiratory illness and 16 control infants without respiratory disease developed CF antibody, neutralizing antibody, or both
- The frequent occurrence of infection when compared with the infrequent “isolation” of “virus” suggested to them that Long “virus” was recoverable from the throat during a very short interval following infection
- They reiterated that Morris, Blount and Savage experienced similar difficulty in “isolating CCA virus” from chimpanzees with respiratory illness
- Chanock et al. admitted that it was an assumption that CF antibody was a measure of recent or persisting infection
- From their findings, they anticipated that infection of older individuals would occur infrequently yet this was not the case
- They offered up possible explanations for this contradiction but concluded that it was not possible to determine which of the alternatives offered the correct explanation
- Chanock et al. admitted that an association between Long “virus” and lower respiratory disease in hospitalized infants was not demonstrable
- Remember how I said to keep in mind the information about the study looking into an association with lower respiratory disease? Chanock et al. point blank admitted that they could not prove such a relationship existed with their “virus.” Game over.
- They felt that such an association could exist but was overshadowed by the high rate of “infection” among the hospital control group
- A definite statement could not be made regarding the spectrum of pathogenicity of Long “virus” for man
- In the majority of infants, “infection” resulted in either mild illness or no discernible disease

In order to accept the discovery of “RSV,” we must ask ourselves a few questions. Is the “isolation” of an invisible agent from one chimpanzee, while failing with 13 others, strong enough evidence to state the existence of a new “virus?” Does the inability to create the same disease in various animals logically lead to the conclusion that the new “virus” was pathogenic? Should indirect cytopathogenic effects in cell cultures and nonspecific antibody results be considered a valid substitute for direct proof of the existence of this “virus?” Is the “isolation” of a “virus” from a single infant by another team of researchers that also relied upon indirect cytopathogenic effects and nonspecific antibody results proof that the two invisible “viruses” are related? Should contradictory results from control experiments be ignored and/or explained away in order to keep the belief in the new “virus discovery” alive? If the original researchers admitted that they could not establish an etiological relationship between their chimpanzee “virus” and illness in humans, what does this tell you about the invisible entity’s ability to cause disease in humans? What if the second group of researchers also admitted to not being able to demonstrate a relationship between their human version of this invisible entity and the lower respiratory disease that they were attempting to associate it with?
To anyone looking at the foundational evidence for “RSV” critically and logically, it is clear to see that no “virus” was ever proven to exist nor cause disease in humans. Instead, we were presented with the same unpurified cell cultured creations, small sample sizes, contradictory results from controls, indirect and nonspecific antibody measurements, and the inability to establish an etiological relationship between the invisible entity and the disease being studied. In other words, just another typical day in the pseudoscience known as virology.

Virology a pseudo science to trick the common man into thinking there’s something out there to be afraid of so then we take their highly toxic injections and other pharmaceuticals which make us sicker .
Very clever , if it weren’t for the fact they are drug peddling murdering psychopaths
LikeLike
It is obvious that no one has ever isolated any so-called atom to be visualized and characterized, which means that there is no real, uninterpretable evidence from which we can conclude that atoms are a reality.
Some claim that although atoms cannot be isolated because Mankind does not possess the technological capabilities to be able to isolate them, this is not proof that atoms do not exist.
Well, if there is no technological capability to isolate so-called atoms, then on what real basis do so-called scientists claim that atoms exist?
Just as it is with the so-called atoms, so it is with the so-called molecules.
No one has ever isolated any so-called molecule to be visualized and characterized, which means that there is no real, uninterpretable evidence from which we can conclude that molecules are a reality.
Of course, existence is also structurally intelligent in the sub-microscopic realm, that is, beyond the visible realm.
But what goes beyond the visible realm also goes beyond the limits of human perception and understanding.
The man who refuses to recognize that there are great natural limitations to human capacities for perception and understanding of existence… is driven by selfish and destructive soul-feelings.
——————————-
Hebrews 11:3
It is by faith we understand that the whole world was made by God’s command so what we see was made by something that cannot be seen.
———————————
„Today’s scientists have substituted mathematics for experiments, and they wander off through equation after equation, and eventually build a structure which has no relation to reality.”
– Nikola Tesla
——————————–
„All matter originates and exists only by virtue of a force… We must assume behind this force the existence of a conscious and intelligent Mind. This Mind is the matrix of all matter.”
– Max Planck
——————————–
„Science cannot solve the ultimate mystery of nature. And that is because, in the last analysis, we ourselves are a part of the mystery that we are trying to solve.”
– Max Planck
LikeLike
I have a leftfield thought that all influenza, measles, RSV phenomena are really attachment strands for bacterial infections.
When working supermarkets for 10 years all the so-called flu epidemics were indistinguishable from strep.
It takes about 15 minutes for someone with a hot cough to make eye watering or throat tickling symptoms if they coughed on you, left unchecked it would cause flu.
But then the DIY treatment that works is generally using any elderflower or elderberry products which stop sialic attachment, with a antibiotic tea like thyme to knock off the strep and you could be OK the next day.
You see sort of studies that indicate the idea.
Respiratory Syncytial Virus Increases the Virulence of Streptococcus pneumoniae by Binding to Penicillin Binding Protein 1a. A New Paradigm in Respiratory Infection
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4226051/
Insights into the Interaction between Influenza Virus and Pneumococcus
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1539103/
Will have to read the blog properly later, ta.
LikeLike
Bacterial infections are a myth too.
Check https://odysee.com/@dharmabear:2/Dr-Thomas-Cowan-What-Makes-You-Sick-WAPF-Oct-22-2022:6
Read https://ia903402.us.archive.org/21/items/2020-thomas-s-cowan-the-contagion-myth-why-viruses-including-coronavirus/2020_Thomas_S_Cowan_The_Contagion_Myth_Why_Viruses_including_Coronavirus.pdf and/or https://odysee.com/cowan-dr-tom-breaking-the-spell:c.
LikeLiked by 1 person
Next, they’ll just say “You have whatever WE say you have. Prove us wrong.” 🙂 Amazing how many “health freedom” activists continue to insist that there really is a unique disease going on out there, too stuck in the narrative to question it.
LikeLiked by 2 people
There are people who regularly say that already to me on Twitter. 🤣
LikeLike
Truly, nothing left to do bu 🙂 🙂 🙂
LikeLiked by 1 person
This is right on time. I’ve been talking to a number of people I work with about symptoms and how that doesn’t mean you have a virus. I’m going to be referring people to this site for technical information. In the meantime I’m still busy working on it from a theological perspective. If you get time read this thread where I just got finished on Reddit with a number of “religious” people about vaccines. The stopped allowing comments but the thread is still there.
LikeLiked by 1 person
Sounds interesting. I’ll give it a look! 😀
LikeLike
Or, too arrogant to admit they were wrong. Or cognitive dissonance has gotten the better of them. Or, they are paid by governments or big pharma and will spread any narrative they are paid to spread. Do not estimate the amount of corruption and controlled opposition.
LikeLiked by 1 person
The title of the post was “information for those seeking spiritual clarity on the subject of COVID-19 vaccination.” The post simply had a link to an article I posted on my website about the subject. I posted it on a Lutheran subreddit, an Episcopalian, a Baptist, a Mormon, a Seventh-Day Adventist, a Jehovah’s Witness, and a website that deals with issues pertaining to Jesuits in the Catholic Church—seven subreddits in all, with over 6,000 views and seven link shares to I don’t know where. The post was only deleted at the Episcopalian subreddit. That’s when I posted the other message, “Who gets to decide?” That post was the one that got the fireworks started. Both the people, the moderators, and a religious leader admitted that they all believed in viruses and had been following the advice of the medical professionals, as can be seen from the post. Although a fair amount of my response was deleted, it is obvious that these people had done no research.
In my article, I tried to keep things as simple as possible without going into too many technical details and medical terminology, except for some of the quotes that I made from reference material. It was good to see that the people understood what I was saying, even though they vehemently disagreed with it. Hopefully, they will hear this same story from other sources, begin to question why they believe what they’ve been told, and start to do their own research.
Mankind has a spiritual nature, and making the virus issue a spiritual matter has given it the extra attention I think it deserves. But it is still absolutely necessary to back up the claims against virology with facts, and Mike and others play a very important role in that effort. It would not be possible to refute it on a spiritual level without facts from the material world.
LikeLike
Thanks Mike. Great work..
Explained via GNM
https://media2-production.mightynetworks.com/asset/50382281/RSV___respiratory_syncytial_virus_.pdf?_gl=1*164nb9p*_ga*MTIzMTkzOTQ4OC4xNjI1NzM1OTcw*_ga_T49FMYQ9FZ*MTY3MTIzMDQ1MS4xNjY0LjEuMTY3MTIzMDQ1NC4wLjAuMA
LikeLike
While I think GNM has some merit, I also feel that it goes too far in explaining pretty much every ailment as a psychological conflict, and thus diminishes the role that diet, cosmetics, pollution and radiation play. To me, each ailment has a physical and psychological component, where the ratio varies from person to person, from ailment to ailment.
LikeLiked by 1 person
I agree 💯
LikeLike
People who destroy lives, as well as the possiblility of delaying/finding actul truths deserve to be theorized as the dangers they are. That should always accompany consequences.
LikeLiked by 1 person
New virus equals new vaccine—that’s the equation they use to make money. Some are even saying there is a hidden agenda here to reduce the population. If that is true, then what better way to target mother and child at the same time?
Researchers on cusp of rolling out new vaccine for RSV
BALTIMORE —
Researchers are on the cusp of rolling out a new vaccine to combat respiratory syncytial virus amid an increase of cases in recent months. . .
. . .”It will be a huge, huge breakthrough for us to have an RSV vaccine available,” said Dr. James Campbell, professor of pediatrics and the University of Maryland School of Medicine. . .
. . .Moderna released preliminary results of their vaccine for RSV that shows it’s more than 80% effective at preventing serious disease in people older than 60. The company is preparing to submit the vaccine to the Food and Drug Administration for approval, which follows submissions from Pfizer and GlaxoSmithKline late last year. . .
. . .”The Pfizer vaccine, they also relayed results on giving that same vaccine to pregnant women, and then what happens is the antibodies the woman makes, gets passed through the placenta into the baby, and they showed very good protection in the first three months of life,” Campbell said. . .
. . .Clinical trials are underway on a vaccine for babies and young children, who are among the high-risk groups for developing complications and dying from RSV. . .
. . .These would be the first RSV vaccines approved, which would be a feat because researchers have been working on them since the 1960s. Moderna’s version uses the mRNA technology made famous by its COVID-19 vaccine. . .”
https://www.wbaltv.com/article/moderna-rsv-vaccine-study/42589008
LikeLiked by 1 person
Bingo! They did the same with monkey pox. 😉
LikeLike
It’s getting worse.
Doctors are increasingly making diagnoses using information from computers controlled by global players
“Surely you have noticed a worrying trend over the past few decades. When you see a doctor, they seem to spend more time looking at their computer than questioning or looking at you. That’s because the Department of Health has them connected to databases where they can enter symptoms and ask the computer what tests to run and what pills to prescribe.
Authorities, politicians and doctors have increasingly placed themselves in the hands of information delivered directly to their computers by operators with commercial and political intentions. Many of these operators operate in a global space outside the confines of national regulation, and they directly control medical agendas via sophisticated databases that relay suspicious information. . .”
https://uncutnews.ch/aerzte-diagnostizieren-zunehmend-mithilfe-von-informationen-aus-computern-die-von-globalen-akteuren-kontrolliert-werden/
LikeLiked by 1 person
Reblogged this on BertieS.
LikeLiked by 1 person
Thank you! 🙂
LikeLike
Many of those symptoms in the list could also explain a common cold or any variety of cold. I figure big pharma has never come close to inventing a vaccine for the common cold, which I believe is of the rhinovirus type and that is vexing.
How could we ever expect them to invent a potion for covid, also a rhinovirus? It stinks to high Heaven, I think. With colds being the most common form of tame illness, you would think big pharma would have come up with a vaccine by now.
After all, cold germs or viruses must be everywhere on the planet. Or, perhaps they are nowhere and that is why big pharma cannot make a vaccine.
LikeLiked by 1 person
They can not eliminate these common symptoms, and they know it, which is why there will never be an effective common cold vaccine. They can only convince people that whatever injection they received protected them from hospitalization and death.
LikeLike
Your reasoning implies that vaccines are made to protect and heal. They are not. They are chemical weapons, created to make people sick. If they get sick, they will get “medication” to treat that illness. Make no mistake, vaccines are anti-human in nature.
LikeLiked by 1 person
I think he is looking at it from their point of view. If you really get down to it, there should be no word for virus because viruses aren’t real, unless you want to use the word to describe something fictitious. It is the same with vaccine. There are no vaccines because they can’t do what they say they do. It’s fiction.
LikeLiked by 1 person
The mythology of the lying atomist-molecular sciences (chemistry, molecular biology, genetics, virology, immunology) has no relation to the True Art of Healing.
I refuse to continue to believe, unconditionally, the claims of those who consider themselves scientists (based on the credentials they receive from financiers, politicians and militarists) that atoms and molecules exist, even if there is no direct (uninterpretable) evidence.
What disgusts me most about self-proclaimed scientists is the infamous way they manipulate people’s blind credulity by appealing to so-called scientific authority and so-called scientific consensus and issuing an endless number of supposed scientific explanations using a language specifically designed to make people think that science is only for geniuses.
There is a popular saying that there are no more brainwashed, stupid, ignorant and arrogant people than those who have degrees.
————————————-
“The course of every intellectual, if he pursues his journey long and unflinchingly enough, ends in the obvious, from which the non-intellectuals have never stirred.”
– Aldous Huxley
LikeLiked by 1 person
On the fraud that genetics is, have you read https://criticalcheck.wordpress.com/2021/12/15/dna-discovery-extraction-and-structure-a-critical-review/?
LikeLiked by 2 people
When a so-called scientist talks about electrons, protons, neutrons, atoms and molecules as something that really exists, that so-called scientist is either a big liar and a big fraud, or a big brainwashed.
LikeLike
…or a combination of those. 😉
LikeLike
I would like to state that questioning the foundation of virology should not be turned into a movement/our experts/my team type of mentality.
LikeLiked by 1 person
I’m new to the questioning of whether or not viruses are real or not. But one question I get is “well if viruses are not real, then what causes people, (and more specifically babies/children) to get sick?”
The natropathic doctor (of which I am not) would say, that the baby is growing. The slothing off of dead endothelial cells need somewhere to go. The bacteria comes in to eat it and the body must eject the waste.
This started to make sence to me the past fall into the winter. In Canada the RSV episode was paired with a Tylonal shortage. Parents were hindering the God-given immune response slowing the body’s ability to excrete waste. The primary infections were prolonged the waste didnt leave as it should have and as a result secondary infections emerged.
Once again we see fear as the victor, as the result of our cultural brainwashing which tells us to fear sickness and fevers. Once again we turn our backs on the our Creator and His perfect design. For I know the plans I have for you,” declares the Lord, “plans to prosper you and not to harm you, Jeremiah 29:11.
LikeLike
Here’s a great intro into what makes you sick:
https://odysee.com/@dharmabear:2/Dr-Thomas-Cowan-What-Makes-You-Sick-WAPF-Oct-22-2022:6
https://odysee.com/@dharmabear:2/Sally-Fallon-Morell-Contagion-Myth-Session-2:5
We don’t need the germ model to explain disease when we are surrounded by toxic food and drinks, poisonous cosmetics, elektromagnetic radiation and lots of stress.
Awesome docu on germ theory:
https://odysee.com/@spacebusters:c9/Final-The-End-of-Germ-Theory:8
LikeLiked by 1 person
I had a niece and two employees in the past 6 months who have had babies, each of the 3 babies was diagnosed with RSV within 3 months of birth, 2 were admitted to the hospital, one for 4 days. Each of the mothers had been vaccinated, and 2 were boosted during pregnancy. All three believe their babies caught a virus, yet all three said no others in their family were sick or got sick. Fascinating mindsets.
LikeLiked by 1 person
Yes, it is truly fascinating what people can convince themselves of despite what the evidence clearly shows.
LikeLike
Maybe send them Breaking the Spell?
https://odysee.com/cowan-dr-tom-breaking-the-spell:c
It helped me wake some people up. Remember, they are just afraid for their babies, which is only natural for a mother.
LikeLiked by 1 person
Now this is interesting. I would love to be in the courtroom to see how the “evidence” is introduced in this case.
13 women plan to sue Houston building owner after they say they got herpes from janitor
Lucio Catarino Diaz is charged with aggravated assault with a deadly weapon. Court records say the deadly weapon is his bodily fluids which contain the herpes virus.
HOUSTON — Thirteen women who all claim to have contracted an incurable STD while at work from a janitor who tampered with their water bottles are filing suit against multiple companies who they say disregarded the janitor’s behavior.
https://www.khou.com/article/news/local/lawsuit-to-be-filed-after-women-allegedly-contract-std-from-janitor-houston/285-56c2f776-11c5-4bbe-ab2e-1b98d68792a1
LikeLiked by 1 person
You do realize who controls the court room, right? 😉
https://odysee.com/Government–The-Biggest-Scam-in-History–Exposed_backup:9
LikeLiked by 1 person
Of course, the judge – an agent of the state. Don’t forget the “expert” witnesses. Funny thing though, you can’t be a judge or an expert witness unless you stay within the matrix they’ve constructed for you to live in. If you step outside and proclaim truth then you’re obviously a mental case.
LikeLiked by 1 person
Yes, that would be an interesting case. I would imagine it would be very hard to prove.
LikeLike
They will probably settle out of court just to keep the game going.
LikeLiked by 1 person
No one has ever proved the existence of any atom or molecule. Atoms and molecules are just hypothetical descriptions that so-called scientists have made trying to guess what exists in the submicroscopic realm.
The truth is that electron microscopy, X-ray crystallography, RT-PCR, and all the other laboratory procedures used in so-called molecular biology are all scams.
Naturally, the so-called scientists in the sub-microscopic realm of existence will prefer not to see the truth about the hoaxes they emit and disseminate… and that is to avoid having their consciences reprimanded, to avoid offending The system and not to lose their jobs, functions, social position and material advantages.
LikeLike
Would it be possible if you could make an article about salmonellosis? Even an article about Helicobacter Pylori would be interesting.
LikeLiked by 1 person
Yes, I do hope to get to them. I’ve been exploring bacteria more on my Substack at https://mikestone.substack.com/
LikeLike
Bacteria are our friends. Can’t wait to see you do an article on them Mike! Also make sure to include the infamous legionella. 😉
LikeLiked by 1 person
Hi Mike. It’s me again. Still trying to learn as much as I can. If it’s OK, I have another question. I know that viruses don’t exist so it follows that this poisonous ‘spike protein’ everyone is talking about must have been made in a lab. I think that’s correct.
I recently tried to read this scientific paper:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7439997/
From that scientific paper, my question is this. Theoretically, if someone put some of this poisonous ‘spike protein’ in an injection and injected into people, who would suffer the most ill effects from the poison? Would it be an Ashkenazi Jewish person? Or would it be a European/South Asian person?
I know the covid injections are supposed to make the body produce its own poisonous ‘spike protein’, but I have never really seen any evidence that this is possible.
My learning curve is getting steeper now. I am going to try to understand next generation sequencing as my next project. That should be fun (not!), lol.
LikeLike
Have you seen https://criticalcheck.wordpress.com/2021/12/15/dna-discovery-extraction-and-structure-a-critical-review/ on DNA?
I also found this session with Cowan and Scoglio on the spike protein very interesting:https://odysee.com/@dharmabear:2/Conversations-with-Dr-Cowan-Ep-58-Stefano-Scoglio:e.
LikeLiked by 1 person
Yes, both great resources! Thanks for sharing! 😁
LikeLike
Hi Doris, I’m not positive that the vaccines can target people of different ethnicities. My guess is that they will poison everyone equally, yet as the ingredients may not be uniform, some will be poisoned worse than others. There could be a possibility that they make certain batches more toxic depending on where the vaccines are sent. However, that is pure speculation on my part.
LikeLike
Hi Mike. Thanks for replying. I’m sure you are correct in what you are saying. But I don’t think I asked my question properly. What I MEANT to ask was, what does that paper say would happen if, theoretically, someone put some of this poisonous ‘spike protein’ in an injection and injected into people, would it be the Ashkenazi Jewish person who suffered the most ill effects? Or would it be the European/South Asian person who suffered the most ill effects? I’m asking about the way the poisonous ‘spike protein’ interacts with the ACE2 receptor. I’m not saying the paper is correct. I’m just asking, if it is correct, which race would suffer the most ill effects from the poisonous ‘spike protein. I just don’t understand what the paper is saying. I still have a lot of learning to do.
LikeLike
Doris, you are assuming that “spikes” and “receptors” exist and function the way we are told they do. That too has never been proven. Check out Dr. Cowan’s work on this topic.
LikeLiked by 1 person
I’m sorry I am a bit confused Doris. Which paper are you referring to? I’ve never seen any saying that the vaccine targets a specific race or ethnicity.
LikeLike
I would like to know whether you already made an article about hep A,B,C,D,E ? It would be quite interesting due to the indirect antigen and antibody tests that are used for said conditions. Your articles are more like peer review sessions, which is phenomenal to say the least.
LikeLiked by 1 person
To be honest I think the hep story would be a waste of time. Antibodies are not specific. Hep has never been isolated. It’s pretty much caused by various kinds of poisoning. The rest is the same as with all other “viruses”: it’s bullshit.
Peer review is a circle-jerk.
LikeLiked by 1 person
It would be wonderful to know what these “antigens” or “antibodies” actually represent. Are there studies where specific toxins led to an increase of certain biomarkers in the multitude of indirect “antigen” and “antibody” tests they use? If I’m not mistaken, sars 2 antigen tests even tested positive for orange juice?
LikeLiked by 1 person
Of course any antigen test will test “positive” on other than the intended targets. Reason is that antibodies are not specific. All toxins will lead to an increase of antigens, but that does not mean they are specific. Cowan has addressed this various times in his work.
LikeLiked by 1 person
Thanks! I have not done Hepatitis A-D yet. I did do an old FB post on Hep E but I have not updated it to the site yet. I will see what I can do. 🙂
LikeLike
@Leo Brybor
Hi Leo. Thanks for replying to my post. It may seem like I am assuming that poisonous ‘spike proteins’ and ‘receptors’ exist. But actually I am not. I am obviously not explaining myself properly. All I am trying to do is understand what that paper is saying. I will rephrase my question. Let us ASSUME that poisonous ‘spike proteins’ and receptors DO exist, even though I don’t believe that they do. What I am trying to understand is, what does that paper say would happen if, theoretically, someone put some of this poisonous ‘spike protein’ in an injection and injected into people, would it be the Ashkenazi Jewish person who suffered the most ill effects? Or would it be the European/South Asian person who suffered the most ill effects? I’m asking WHAT THE PAPER SAYS about the way the poisonous ‘spike protein’ interacts with the ACE2 receptor. I’m not saying the paper is correct. I’m not saying poisonous ‘spike proteins’ and receptors DO exist. I’m just asking, IF that paper is correct, (which I don’t think it is), which race would suffer the most ill effects from being injected with the the poisonous ‘spike protein. I’m just asking WHAT THE PAPER IS SAYING. I’m not assuming anything is correct about it. Crikey. I hope I have explained myself properly now. LOL.
LikeLike
“Let us ASSUME that poisonous ‘spike proteins’ and receptors DO exist”
No, let’s not go into their fictional nonsense.
Afaik so far no “weapon” that targets a certain genetic has been developed, but of course my knowledge is limited too. I am open to “prove” that such weapon was created and tested successfully.
LikeLike
@Leo Brybor
I’m sorry, but I don’t understand why I can’t get a straight answer. I don’t want anybody to pretend that spike proteins exist. I’m just asking for someone to tell me WHAT THE PAPER IS SAYING about spike proteins having different effects on different races. IS THE PAPER SAYING that an Ashkenazi Jewish person would suffer the most ill effects from being injected with the spike protein? Or IS THE PAPER SAYING it would it be the European/South Asian who would suffer the most ill effects from being injected to the spike protein? I’m not asking anybody to pretend anything. I’m just asking WHAT THE PAPER IS SAYING. I’m sorry if I did not not make myself clear earlier.
LikeLike
The only thing I wanted to know is WHAT THAT SCIENTIFIC PAPER WAS SAYING. It was purely out of interest. I was not asking if it was true or not. But anyway, I’ve asked a chemist I know and he answered the question for me. It appears that the scientific paper is saying that the so-called ‘spike protein’ is MORE poisonous to European/South Asian people and LESS poisonous to Ashkenazi Jewish people. I believe it’s all nonsense. But it certainly opens the door up to the conspiracy theorists, doesn’t it? I bet they would have a field day with that. lol.
LikeLike
I’m sorry, Doris, I’m still unsure of what paper you are referring to. I’d be more than happy to give an opinion but I’m unaware of the paper you are speaking to.
LikeLike
You made a few articles about the HPV, were you went through the paper by Shope. I am curious to know whether these warts, from the experimental rabbits, induced by the fluids of the wild rabbits, who had warts, contained some sort of toxin. The reason I’m asking this is because of this blog post I read:
https://nourishingtraditions.com/myxomatosis/
LikeLike
I think it’s unfortunate to call exosomes and viruses “the same”, as they clearly do not share the same characteristics – even you can even say that something that does not exist actually has characteristics. More on that in https://odysee.com/@Stellium7:5/is-contagion-a-myth-getting-to-the-heart:3.
You mention “induced by the fluids of the wild rabbits, who had warts,”: how was this proven to be the case? Or is it just an assumption?
LikeLike
I am not sure if there was any toxin as they never look. Just the process of scarification of the skin of the rabbits alone may have been enough to create warts. Sadly, no other alternative explanations are ever examined.
LikeLike
I assumed it, but there must have been some sort of toxin(s) that led to these odd looking warts( not saying that shope proved a virus caused it). It would be interesting to unravel the mystery of what causes these warts.
LikeLike
“but there must have been some sort of toxin”: agreed, but that toxin likely came from within the body, and the warts are a mechanism of trying to get rid of it, kind of similar to a tumor.
LikeLike
Super-resolution microscopy ditches fluorescent tags for gentler imaging of live cells
“. . In one demonstration, they examined features only 86nm in size in living yeast cells. The researchers call the technique photothermal relaxation localisation or Pearl microscopy. . . ”
https://www.chemistryworld.com/news/super-resolution-microscopy-ditches-fluorescent-tags-for-gentler-imaging-of-live-cells/4016926.article#
LikeLike
@Mike Stone. Mike, I don’t know why some messages have ‘Reply’ links here and some don’t. So, for clarification, I am replying to this post of yours.
“I’m sorry I am a bit confused Doris. Which paper are you referring to? I’ve never seen any saying that the vaccine targets a specific race or ethnicity.”
This is the paper I am referring to:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7439997/
I was not saying any vaccine targets any specific race or ethnicity. I was asking a ‘theoretical’ question based on that paper. You will see the question repeated several times in my previous few posts here. One person here actually declined to answer it because it was only ‘theoretical’. I was only trying to learn. I did not imply that anything was either true or false.
I’m sorry for the confusion. Keep up the great work. Love from Doris. x
LikeLike
No worries Doris. It looks like they just compared sequencing data using mathematical estimations in order to create their own fictional narrative. In other words, same old same old. 😉
“Classical electrostatic calculations based on solving Poisson-Boltzmann (PB) equation are used to investigate the interaction energies between SARS-CoV-2 and ACE2 for different mutated ACE2 structures.”
“In an attempt to better understand the susceptibility of different populations to infection by SARS-CoV-2, we gathered data on ACE2 missense variants from different projects and databases that aggregate allele frequencies (AF).”
LikeLike
That is all assuming that what we are told on ACE2 is true, which has never been proven. 😉
LikeLiked by 1 person
When you link articles please link the full version, not something behind a paywall that only shows abstract and conclusion.
For your article: https://sci-hub.ru/10.1016/j.bbrep.2020.100798
LikeLike
What do you think, Mike? Fig. 3: Cryo-electron tomograms of platelets alone and in the presence of SARS-CoV-2 S protein on a collagen I support.
https://www.nature.com/articles/s41467-023-36279-5/figures/3
LikeLike
I only have one question.
Is the spike protein synthetic, which means it was created in a lab, or of natural origin?
Now I may be wrong about what I have to say about this matter, and at the risk of being in error, I’ve concluded the following, at least for now.
A platelet is 1.5 to 3 microns in diameter, which is 1500 to 3000 nanometers.
What are called virions are close to 100 nm. The spikes protrude from the virion and are smaller, probably around 10 nanometers. So called virions are artifacts produced by the EM process. None of these particles have ever been observed in a living cell.
Using the lower size of 1500 nanometers for the platelet and 10 nanometers for the spike yields a ratio of 150:1. It will take 150 spikes to fit across the diameter of the platelet end to end.
What is alleged to be a spike in the images appears far too large to be a spike from what is called a virion. (Extracellular vesicles are often called exosomes, virions, or virus-like particles.) Cells produce spikes on their surface when they shed their membrane. These spikes are not the same as spikes on virions. Cryo-EM causes disorder in the water, yet the claim is made that the 3-D structure is retained. But there is no unfrozen 3-D structure to compare it to, since the cell is no longer alive when imaged. The freezing cannot be harmonious. It must travel from the surface of the structure to Its center. The mass is also less towards the center and must react differently than the larger mass at the surface to the freezing process. There is simply no way to determine what artifacts are produced by this process. The appearance of spikes may be a result of membrane shrinkage however instantaneous. Platelets also contain various granules with numerous active substances. These may also have something to do with what is seen on the images. I think what is called the evidence for the existence of a spike protein has undergone spoilation and is therefore inadmissible.
LikeLike
Yes George, the spike protein is synthetic, it was created in silico, meaning in software.
Have a look at the great explanation by Stefan Scoglio in https://odysee.com/@dharmabear:2/Conversations-with-Dr-Cowan-Ep-58-Stefano-Scoglio:e.
LikeLiked by 1 person
Hi George. According to Stefano Scoglio, the ‘spike protein’ everyone is talking about is ‘recombinant spike protein’ not natural ‘spike protein’. I am assuming that ‘recombinant spike protein’ is man-made in a laboratory. However, I still don’t know if any actual real physical samples of this ‘recombinant spike protein’ exist anywhere in a test tube or something. Or is it all just in-silico nonsense like it usually is? Do you know which it is, George? I am finding this stuff really difficult to understand lately. Maybe because it’s all fake. lol.
LikeLike
Sure it exists, as you can buy it online. Why does this matter.?
LikeLike
“in the presence of SARS-CoV-2 S protein”: how was this determined, other than by matching a man-made in-silico sequence?
Was a control experiment done?
“Source data are available as a Source Data file.”: do you have that data?
Looks like a lot of fancy cgi again, combined with pictures where someone says: “this is the spike protein.” – sure, ok, how do you know that? How do we verify that?
Did you see https://odysee.com/@dharmabear:2/Conversations-with-Dr-Cowan-Ep-58-Stefano-Scoglio:e?
LikeLiked by 1 person
Hi Leo. I am getting really confused here. In the first five minutes of that Tom Cowan/Stefano Scoglio video you linked to, Stefano Scoglio stated that all the spike protein they use is synthetic recombinant spike protein. So I assume this synthetic recombinant spike protein is an actual real substance that exists in a laboratory somewhere, and not just an ‘in-silico’ model that only exists in a computer. Am I correct in assuming this? I’m sorry, but I’m not understanding things very well lately. I don’t know why.
LikeLike
Yes, your assumption is correct. The “spike protein” is synthetic genetic material, which does exist, but not out there in nature. Does that help clear your confusion?
LikeLiked by 1 person
@Leo Brybor. Hi Leo. I’m sorry I posted an article that was behind a paywall that only shows abstract and conclusion. But, in my defence, I am not a scientist and I could not tell the difference between a full article, an abstract and conclusion, and a hole in the ground. This ‘science’ business is a learning experience for me. However, if you want to buy a combine harverster, a tractor, or twenty tons of complimentary sheep feed, then I’m your woman.
LikeLike
No worries Doris, I only meant to show you how you can view articles you normally pay for, through https://sci-hub.tf/ for free. Most articles are paid, since “they” do not want lesser mortals like you and me, the “uneducated baffoons”, to read what nonsense they are writing amongst each other. 😉
Spread the word, as not many people know about the Sci-Hub effort yet.
Let’s learn together!
LikeLiked by 1 person
Thanks Leo. I will use sci-hub in the future. Actually, whilst I’m here, I do have a question. Do you know if anyone has ever actually physically synthesised this so-called ‘spike protein’ in a laboratory? I mean, are these people claiming that there are actual physical samples of this alleged substance in a laboratory somewhere? Or are they just talking about their usual ‘in-silico’ nonsense? The reason I ask is because I have seen people talking about patents for it. But I may have got it all wrong. I know you were talking about it earlier. But I didn’t really understand exactly what was said. Thanks. Doris. x
LikeLike
Hi Doris, here’s an example of where you can buy the synthesized “spike protein”: https://www.sinobiological.com/category/cov-spike/proteins.
LikeLike
On the topic of H.pylori, the two microbiologists ,who allegedly found the bacterial cause of stomach ulceration , had an odd way of proving causation were one of the microbiologist drank a toxic soup( he obviously developed stomach ulcers) to prove the bacteria caused his ulcerations. Has anyone read this paper?
LikeLike
Link? Why would we waste time on it? 😉
LikeLike
“After vaccination, the mRNA will enter the muscle cells. Once inside, they use the cells’ machinery to produce a harmless piece of what is called the spike protein. The spike protein is found on the surface of the virus that causes COVID-19.”
This is what they claim to be the way a spike protein is produced.
1) There are no viruses. Therefore, nothing in nature can cause the production of the alleged Spike protein.
2) They claim the cells have something called ribosomes and these are said to contain the machinery that is hijacked by the mRNA in the lipid nano particle.
3) Ribosomes are a theoretical construct. There is no proof they exist or function as they claim.
4) There is no proof that there is any biological material in the lipid nanoparticles.
5) since the lipid nanoparticles have been proven to be cytotoxic, then they are capable of causing spikes on the membranes of dying and disintegrating cells. Some extracellular vesicles that are shown on EM images show spikes on their surface, but these spikes are the result of the breakdown of the cells and the preparation involved for the imaging in electron microscopy. They don’t prove anything.
Despite numerous pictures hanging in local post offices, so far the notorious spike protein has not been apprehended.
LikeLiked by 1 person
Hi George. Thanks for replying. OK. I accept there is no valid scientific proof for the existence of both the ‘natural spike protein’ and the ‘recombinant spike protein’, But I assume that living things must be able to manufacture proteins by some method, whether they use so-called ‘ribosomes’ or not. For example, one of the most toxic substances in the world is a carbohydrate-binding protein called ricin. Do we know how the castor bean manages to make that? And also, how do we know exactly what is in these so-called ‘vaccines’? Has anyone ever been able to perform complete qualitative and quantitavive analyses of these so-called ‘vaccines’? I’d better leave it there for now. I don’t want to ask too many questions at one time.
LikeLike
I don’t know much about proteins. I know I get a lot of protein in my food. Maybe the cells take in protein and release excess protein? Or modify it in some way?
I’m not going to say much about the vaccines at this point. But, whatever is being used must be something available from the current state of technology. Please consider this article.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2676811/
LikeLike
The bottom line is that “science” is clueless on how proteins come into existence in our bodies. All we know for sure is that what “they” are telling us, is nonsense. As Dr. Cowan says often: science is about figuring out what isn’t true, as that will eventually lead you to the truth.
LikeLiked by 1 person
Exactly George, totally agree! It has not been shown even once that the “spike protein” enters the cells, let alone gets “manufactured” by the (nonexisting) ribosomes.
More on that is in https://odysee.com/@dharmabear:2/Conversations-with-Dr-Cowan-Ep-58-Stefano-Scoglio:e.
LikeLiked by 1 person
@George. Hi George. I appreciate your comments. I always like talking to you. I don’t think I will say much more about the so-called ‘vaccines’ either. I have my own ideas. But I don’t want to get Mike’s website shut down, so I won’t say anything else here. Look after yourself, my friend. I wish you all the best.
LikeLike
This doesn’t pass the smell test.
“. . . But, unlike the other vaccines, Novavax directly injects a version of the spike protein, along with another ingredient that also stimulates the immune system, into the body, leading to the production of antibodies and T-cells. (It injects a version of the spike protein that has been formulated in a laboratory as a nanoparticulate that does not have genetic material inside and cannot cause disease.)
“I often tell people, imagine an eggshell without an egg in it. That’s what it is,” Dr. Wilson says.
The Novavax vaccine is a traditional one compared to the other vaccines. Its technology has been used before in vaccines to prevent such conditions as shingles, human papillomavirus, and DTaP (diphtheria, tetanus, and pertussis), among others. . .”
https://www.yalemedicine.org/news/novavax-covid-vaccine#:~:text=The%20Novavax%20coronavirus%20vaccine%20(brand,40%20other%20countries%2C%20including%20Canada.
“another ingredient that also stimulates the immune system”
I wonder what that could be?
Traditional vaccines are made using a cell culture. It doesn’t sound like this is what they are doing. It looks like they are saying the spike protein is inside a lipid nanoparticle instead of mRNA. I’ve not seen proof of mRNA in the others and I would like to see proof of the presence of the elusive spike protein in this so-called traditional vaccine. I don’t believe there is a difference between this vaccine and the others. I think they’re all loaded with PEGylated graphene oxide nanoparticles.
They also say this technology has been used before for other so-called viruses. At some point they must have made a change, if what they are saying is true, because traditional vaccines use adjuvants. Who knows, maybe they mean PEGylated graphene oxide nanoparticles are adjuvants. The distinction is that the other adjuvants used in the traditional vaccines were not nanoparticles.
LikeLiked by 1 person
Why so secretive about the other ingredient? It is rather odd to even include that information if they were not going to say what it is.
LikeLike
Last year I sent a FOIA request asking for the complete nucleotide sequence for the mRNA alleged to be in two of the vaccines. They would not tell me. They said it was protected information. So it is not unusual for them to keep things a secret.
I also found this article in their literature. If I posted these ideas it would be considered disinformation. Even their own literature raises serious questions about their products.
Questioning the Use of PEGylation for Drug Delivery
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4051498/
LikeLiked by 1 person
According to the so-called science, the mRNA contained in the covid vaccines is supposed to stay in the muscle. I assume, according to their “science,” this claim means the ribosomes in the muscle cells will be used to produce the spike proteins. However, aside from the unproven replication theory, which is alleged to be a function of something called a ribosome, I believe there is an additional problem.
In his interview with David Crowe, Dr. Harold Hillman claims (at least to my understanding of the conversation) muscle cells do not contain what are called ribosomes, which he says are granules, whose shape cannot be determined because they are so small (approximately 20 nanometers). Apparently, he believes muscle cells do not contain what are claimed to be ribosomes, because the granules, normally seen in cells, are not seen in muscle cells under the election microscope. This gives rise to the question, “why do virologists claim muscle cells contain ribosomes, if the granules imaged in most cells are not imaged in muscle cells?”
In addition to what is seen under electron microscopes, virologists use the artifacts obtained from cryo-electron microscopy and x Ray crystallography to claim ribosomes exist in living cells and mediate protein synthesis and viral replication. Yet there is no direct evidence to support this claim. They use these two procedures to correlate their results with the artifact imaged under the electron microscope.
At the 24:00 minute mark, which is a little messed up due to audio problems, the topic of ribosomes is discussed. The podbean app is required to listen to it.
https://www.podbean.com/ea/pb-m5it3-4ef14c
There is also a great deal of other valuable information discussed in this interview.
LikeLiked by 1 person
Interesting! Can you link this on Odysee?
LikeLike
I don’t know what odysee is or how to do it. I am pretty stupid when it comes to such things. I grew up when there were no computers, no internet, and no cell phones. In fact, when I picked up the phone sometimes I heard my neighbor talking on it. We had what was known as a party line. For the sake of expediency, copy it and do what you would like to do with it.
LikeLiked by 1 person
https://infectiousmyth.podbean.com/e/infectious-myth-we-can%e2%80%99t-trust-our-eyes-052814/
If you go to that link on a PC, you can just listen to it without having to download any ‘apps’ or anything like that.
LikeLiked by 1 person
Actually Doris, when I go to that link, I can play it in my browser just fine: just click the orange play button.
LikeLike
Thanks, good to know.
LikeLike
From what I understand, and I might be wrong about some of this, in Biblical times, people would go to visit a sorcerer with the goal of being healed or protected by means of drug-mediated effects. The drugs, administered by the sorcerer, were thought to be able to mediate a healthy condition in the recipient. The sorcerer often mixed various ingredients into a potion. The potion was simply a drug. Sorcery is sometimes translated as druggery. This is not spiritism because the sorcerer is not acting as a medium between his patient and the spirits, although he might engage in spiritism during the same visit.
The sorcerer had no idea how the body functioned, nor did he understand how his potions would affect his patient. So things were pretty much guaranteed to go wrong. This is why sorcery was often associated with poisoning. Nevertheless, people were desperate enough to try anything when they were suffering from an unhealthy condition.
Under the terms of the law covenant, persons involved in sorcery were often characterized as becoming unclean or defiled. This designation was given to call attention to the spiritual defilement that resulted from transgression of the law; nevertheless, physical damage would also result from the transgression as well. In this way, the sin planted the seed of its own punishment.
It is possible that individuals might have attributed the damage from the drugs as a progression of the original disorder and not as a result of the attempt to treat it. In this way, they might have been willing to visit the sorcerer for a second dose, or a “booster,” if you will.
In conclusion, it is worth noting that the Bible uses fairly strong language about people who visit sorcerers. They were said to have whored after them by being unfaithful to God and rejecting his law. So it was considered a form of spiritual prostitution.
Sometimes I think about these things when I’m banned for spreading disinformation.
LikeLiked by 1 person
That is very interesting George! I love looking back through history to see the parallels to today. It is defintions an area worth exploring more! 🙂
LikeLike
According to the wise man, “there is no new thing under the sun.” I try to keep that in mind, despite technological advancements.
LikeLike
It’s all right here, folks. They knew about the toxicity of graphene oxide nanoparticles before the scamdemic including the corona effect. They studied it in great detail, and then they weaponized it. It is highly probable that the lipid coatings on the particles simply provide additional time for the nanoparticles to distribute throughout the body before they break down and allow the GO to begin its assault at the cellular level.
Toxicity of graphene-family nanoparticles: a general review of the origins and mechanisms
Published: 31 October 2016
“. . . This review collects studies on the toxic effects of GFNs in several organs and cell models. We also point out that various factors determine the toxicity of GFNs including the lateral size, surface structure, functionalization, charge, impurities, aggregations, and corona effect ect. In addition, several typical mechanisms underlying GFN toxicity have been revealed, for instance, physical destruction, oxidative stress, DNA damage, inflammatory response, apoptosis, autophagy, and necrosis. In these mechanisms, (toll-like receptors-) TLR-, transforming growth factor β- (TGF-β-) and tumor necrosis factor-alpha (TNF-α) dependent-pathways are involved in the signalling pathway network, and oxidative stress plays a crucial role in these pathways. . .
. . .GFNs can induce acute and chronic injuries in tissues by penetrating through the blood-air barrier, blood-testis barrier, blood-brain barrier, and blood-placenta barrier etc. and accumulating in the lung, liver, and spleen etc. For example, some graphene nanomaterials aerosols can be inhaled and substantial deposition in the respiratory tract, and they can easily penetrate through the tracheobronchial airways and then transit down to the lower lung airways, resulting in the subsequent formation of granulomas, lung fibrosis and adverse health effects to exposed persons. . .”
https://particleandfibretoxicology.biomedcentral.com/articles/10.1186/s12989-016-0168-y
You can download the PDF and keep it for future reference just in case it disappears.
LikeLike
Just out of interest, is there anyone here who DOES NOT realize that viruses, vaccines, human induced climate change and ANYTHING with the word ECO in it are lies to either control us or kill us.?
LikeLiked by 1 person
“I saw all this when I thought about the things that are done in this world, a world where some people have power and others have to suffer under them.” – Ecclesiastes 8:9, Good News Translation.
LikeLike
The “international bankers” are at the root of all problems in this world.
https://odysee.com/The-Web-of-Debt(audiobook):1
LikeLike
Thanks for all the great articles and videos.
As RSV vaccines have been approved this came up
——-
“The Pandemic is Not Stopping, It Was Too Profitable to Come to an End
When gold was discovered in Otago, people rushed there from all over the world to stake their claim.
We are now witnessing a rush to offer new vaccines and drugs in the hope of huge profits. Pharmaceutical giant GSK is releasing a vaccine it calls Arevxy against common runny nose infection RSV which it says is 94% effective, although the side effects are worryingly familiar.
The target populations are the over 60s and newborns. “Newborns” means that ultimately GSK hopes every baby will have to take it, in other words everyone.
The UK Sun leads with ‘JABS UP Millions to get vaccine to protect against ‘fatal’ virus that lives in 90% of Brits – are you eligible?’ promoting the Shingrix vaccine already available here in New Zealand. Good job they put the word “fatal” in inverted commas, Shingles almost never is.
Although enjoying the title “vaccine,” Shingrix doesn’t actually prevent shingles, instead it is claimed to reduce the symptoms. Sound familiar?
These claims pale by comparison with those offered by Harvard scientists who announced they have discovered the elixir of youth consisting of six chemical cocktails which reportedly helped mice skin cells survive a little longer. Very timely really, considering human population longevity is rapidly reducing probably due to other chemical cocktails we are regularly given in our food and medicines.
Exaggerated tales of golden reefs were no strangers to the gold fields where disappointed miners tried to sell their dud claims to newly arrived prospectors. The idea that a chemical cocktail is going to lead to eternal life is a tired narrative that is past its sell by date.
The huge gains in longevity we enjoyed during the last century were due to hygiene and nutrition, not to pharmaceutical concoctions. Don’t be tempted to swap the benefits of a natural varied diet for the promises of a pill salesperson.
The medical gold rush is going nowhere except down the drain.
I am hoping you will join me in asking again and again, why are our hospitals overwhelmed? Why are excess deaths at unprecedented historical highs? Why are our politicians, medical professionals, and media remaining silent? Why are thousands injured by vaccines being gaslighted and ignored? Why is the government still telling the public it is essential to keep on getting covid vaccinations and many other novel biotech cures? The longer this goes on, the more criminally motivated it all appears.”
——
Nirsevimab, which will be sold under the brand name Beyfortus, is not a vaccine. Vaccines prompt the body to make antibodies to defend against pathogens. Instead, nirsevimab is a form of passive immunity. It’s a ready-made antibody that can bind to the virus and block it from infecting healthy cells.
The immune system doesn’t have to make anything.
“The antibody in nirsevimab has been stabilized so it lasts longer in the body — four to six months — and it seems to be more potent.
It’s approved for use in all infants, even healthy infants born full-term”
“Nirsevimab may not be the only option for preventing the infection this fall. The FDA is weighing whether to approve Pfizer’s vaccine for pregnant women that would also protect babies. In that case, the mom makes the antibodies, which cross the placenta to safeguard the fetus and are expected to last through an infant’s first few months of life.
That vaccine would protect babies from the moment they are born, a benefit if the infection shows up out of season. Vaccines also prompt the mom’s body to make more than one kind of antibody, which would provide broader-spectrum protection”
https://edition.cnn.com/2023/07/17/health/rsv-antibody-nirsevimab/index.html
——
Insanity how they can come up with such a convoluted way of thinking.
The “good “ news is one does not need the immune system model anymore as the immune system will come through a needle.
LikeLiked by 1 person