
Differential Diagnosis?
“It’s probably viral, and it just needs to run its course.” 🤷♂️
differential diagnosis
: the distinguishing of a disease or condition from others presenting with similar signs and symptoms
https://www.merriam-webster.com/dictionary/differential%20diagnosis
I imagine most of us have “fond” memories of going to the doctor when feeling unwell and getting subsequently poked and prodded in order to determine a “cause” for the illness. Beyond checking for a fever with a thermometer, the examination performed usually involved a listen to the lungs and heart with the stethoscope, the use of a thick wooden popsicle stick pressed to the tongue to examine the throat, a look into the nose and ears with the otoscope, and a feel of the glands around the neck to check for inflammation and swelling. Unless a strep test (which consisted of a long q-tip being swirled in the back of the throat) was called for and came back positive, more often than not, we were sent home without any testing or medications with the sage advice that “it’s only a viral infection and it just needs to run its course.” Essentially, the only purpose of the examination was to get the written doctors note for school the next day. We were left with the warm and fuzzy feeling that the doctor had absolutely no idea what was going on and the best cure was Grandma’s timeless remedy: bed rest, chicken noodle soup, and ginger ale.
A 2015 article reprinted in The Washington Post by Chad Hayes, a resident physician in pediatrics in Greenville, S.C., discussed this very common scenario. In his article, Hayes admitted that in most cases, testing is not performed as there are no differences in the treatments given for any of the resulting symptoms assumed to be caused by different “viruses.” As they do not want the patient to feel like they wasted their time, doctors offer complex sounding medical terms to the patient which essentially all mean the same thing: it’s just the common cold and the doctor has nothing else to offer:
Your kid is really sick, but the doctor says it’s ‘just a virus’
“Of course, when your pediatrician diagnoses your child with “just a virus,” he’s implying that it’s one of those that doesn’t typically cause much harm. There are thousands of viruses out there that can cause cold symptoms, and we don’t tend to test for them. It would be ridiculously expensive, it wouldn’t change what we do and you probably wouldn’t get the test result until the symptoms had gone away.
“Just a virus” is also implying that it’s a problem he can’t do much about. In contrast to bacterial infections, which are typically treated with antibiotics, most viral infections are stomped out by your immune system in a few days. Antibiotics don’t do a thing to treat viruses.”
“If you do take your child to the doctor for a virus of the “just a” variety, she may be diagnosed with a “viral syndrome,” “upper respiratory infection” or “acute viral rhinitis.” These are doctor terms for “a cold.” (When you go to the trouble of bringing your child in, we don’t want to seem like we are downplaying your concerns, so we use a complicated medical term instead of “a cold.”)
After making this diagnosis, the doctor will probably provide reassurance and recommend “symptomatic care.” This means fluids, rest, humidifiers — things you were probably doing already. I promise, it’s not that we don’t understand how miserable “just a” viruses can be. Trust me, we’ve all picked up more than our share from snotty little kids (including our own). It’s also not that we don’t care. It’s just that we have nothing else to offer.
But don’t worry. It’s just a virus. He’ll be fine.”
Why is it that physicians can not provide anything more concrete when examining symptoms rather than the slogan “it’s just a virus and it will run its course?” It’s because they can not clinically diagnose any disease based on symptoms alone as the different conditions said to be caused by distinct “viruses” all share many similar and overlapping presentations. Try as they might, it is impossible to distinguish and definitively diagnose someone clinically with a specific “virus.” Hence the need to offer complex sounding medical terms to cover up the ineptitude.
Knowing that clinicians can not differentiate and diagnose between disease processes based on symptoms alone, an article published in Science-Based Medicine discussing the possibility that an uptick in “Covid” cases in 2021 was possibly due to a misdiagnosis of “Covid” with RSV immediately caught my attention. As we are currently said to be in the midst of a “Tripledemic” involving RSV, influenza and “SARS-COV-2,” I figured it would make for an interesting read, especially as it is well known that clinical diagnosis of “Covid-19,” influenza, and RSV is impossible, hence the need for molecular tests such as PCR. This was pointed out in July 2021 by Dr. Gregory Poland, an infectious diseases physician and researcher at Mayo Clinic, who stated: “You cannot distinguish them just by clinical symptoms, unless you had the loss of taste and smell, which would push you toward saying, ‘Well, this is likely to be COVID.’ The only thing you can do is the swab nasal test to distinguish the infection.” Apparently, Dr. Poland is one of the few who still believe anosmia is specific to “SARS-COV-2” when it is anything but specific or unique:
“Although a loss of taste and smell is often considered to be a symptom unique to Covid-19, other viruses, including those that cause the common cold and flu, can affect someone’s sense of taste and smell.”
https://www.advisory.com/daily-briefing/2022/11/01/virus-comparison
Forgiving his faux pas on anosmia, we can see from Dr. Poland that it is impossible to distinguish between “Covid-19,” RSV, and other respiratory infections based on clinical symptoms alone. The only possibility he allows for in order to distinguish them is by way of fraudulent molecular testing. However, in the Science-Based Medicine article, Dr. Tracey Beth Høeg questioned whether these molecular tests were actually accurate enough to distinguish between “Covid” and RSV or if they were generating incidental false-positives. This tweet by Dr. Høeg, which was suspiciously absent from the article, clarifies her point:

“SARS-COV-2” was being preferentially tested for in the hospital setting at the time while kids were being seen for reasons not attributed to “Covid.” This led Dr. Høeg to believe that an uptick in “Covid” hospitalizations in 0-4 year olds may have been RSV cases instead as this “virus” is said to be more severe than “SARS-COV-2” within that age group. Physicians on social media became furious with Høeg and balked at the idea that they could not distinguish between RSV and “Covid.” The SBM article linked to the below tweet as proof that doctors could confidently distinguish between the two “viruses” based on symptoms alone:

Throughout the article, further tweets from MD’s were presented in support of the little girl waving her finger. Dr. David Levine claimed that “they are completely different diseases and that there’s a test” for them, meaning his criteria for a differential diagnosis is molecular tests, not clinical diagnosis. Dr. Rebekah Diamond MD. tweeted that we have PCR testing to differentiate the “viruses” and then made the false claim that “the diagnosis of has always been clear even before the pcr results.” As “Covid” has never been diagnosed clinically without PCR and there is no way to distinguish RSV from other respiratory infections based on the overlapping symptoms, this seems like a pretty odd thing to claim without corroborating evidence but this is par for the course. The article rightfully pointed out that, in order for a misdiagnosis to occur, pediatricians (who can not diagnose clinically) and labs (which can not get accurate results with fraudulent tests) throughout the country must be abysmally incompetent:
Is RSV Being Misdiagnosed as COVID-19?
“Faced with these numbers, a suggestion emerged that perhaps COVID-19 really isn’t that bad, as children are being overdiagnosed with the virus. I first encountered this idea from Dr. Tracy Beth Høeg, a sports medicine doctor with a PhD in Epidemiology and Public Health. Dr. Høeg wondered on Twitter if the increases in COVID-19 diagnoses were perhaps due to misdiagnosis of RSV:

The observation that prompted Dr. Høeg’s query was, “the 0-4 year olds driving up COVID hospitalization rates recently. 5-17 year olds have decreased/remained stable.” As she explained, a hospitalization due to RSV could be mis-labelled COVID-19 if they have a positive COVID test:

“Pediatricians on social media were justifiably furious at the suggestion that they could not distinguish between these two viruses:

Pediatricians were very confident they could tell the viruses apart on clinical ground alone, in addition to the separate tests that exist for these diseases. RSV is diagnosed with a rapid antigen or PCR test, which is more likely to be used in the hospital setting. COVID-19 is, of course, diagnosed with a PCR test, and false positive tests are extremely rare.
For a child to be mistakenly diagnosed with COVID-19 when they actually have RSV, it would have to mean that their pediatrician is unable to distinguish these diseases clinically, the COVID-19 test would have to be a false positive, and the RSV test would have be to a false negative. Basically, as noted by Dr. Rebekah Diamond, the only way large numbers of children with RSV could be misdiagnosed with COVID-19 is if pediatricians and labs throughout the country were abysmally incompetent:”

Notably, the doctors who now question whether COVID-19 is being misdiagnosed as RSV only consider that COVID-19 is being overdiagnosed, not the reverse. Early this summer when COVID-19 rates were falling and RSV rates were increasing, these doctors didn’t wonder whether COVID-19 was being misdiagnosed as RSV. This is quite revealing.”
While Dr. Høeg was asking relevant questions that anyone should ask, just like the physicians who were out for her blood, she was mistaken in a very important way. In order to misdiagnose “viruses,” the “viruses” in question must be proven to exist first by adherence to the scientific method. This requires a valid independent variable (i.e. purifed/isolated particles to experiment with). However, not a single one of the “viruses” in question have ever been properly purified and isolated directly from the fluids of a sick patient and then proven to cause the symptoms of disease that they are associated with in a natural way. As there are no “viruses,” there is no need to differentiate between diseases based upon fictional “viruses” as the symptoms are all varying stages of the same detoxification process.

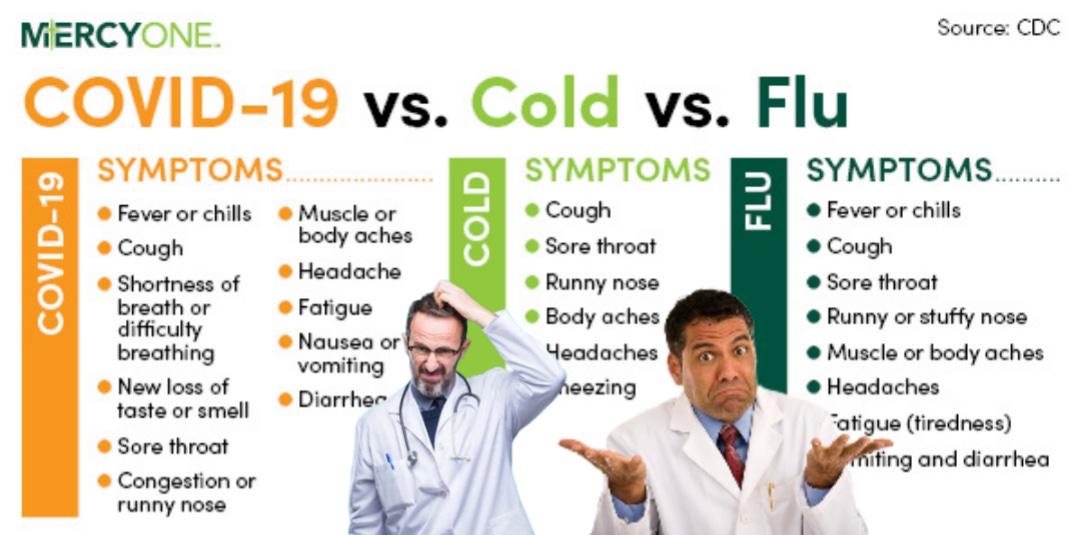
Physicians attempt to differentiate between fictional “viruses” and diseases based upon miniscule variations in symptomology but, as you will see, this is admitted to be impossible as there are no new, specific, nor unique symptoms. Thus, all of the diagnoses attempting to differentiate conditions based on symptoms caused by a specific“virus” are mis-diagnoses.
To highlight this fact, it was known early on in this “pandemic,” as shown in a study published late February 2020, that there was no way to clinically diagnose “SARS-COV-2” and differentiate it with other diseases. The authors stated that this was due to the fact that those testing positive had symptoms ranging from being entirely absent of illness to being severely ill with pneumonia and dying. The nonspecific symptoms which were associated with “Covid-19” were also seen in many respiratory infections said to be caused by other “viruses” and bacteria. Thus, the only way to attempt to claim “SARS-COV-2” as the causative agent in order to obtain a differential diagnosis was by way of PCR testing:
Differential diagnosis of illness in patients under investigation for the novel coronavirus (SARS-CoV-2), Italy, February 2020
“The spectrum of this disease in humans, now named coronavirus disease 2019 (COVID-19) [5], is yet to be fully determined. For confirmed SARS-CoV-2 infections, reported illnesses have ranged from people with little to no symptoms to people being severely ill, having pneumonia and dying [6]. Multiple body tracts may be involved, including the respiratory, gastrointestinal, musculoskeletal and neurologic tracts. However, more common symptoms are fever (83–98%), cough (76–82%) and shortness of breath (31–55%) [6,7]. These nonspecific symptoms are shared by many other frequent infectious diseases of the respiratory tract caused by bacteria and viruses, most of which are self-limiting but may also progress to severe conditions [8,9]. Among these, the most relevant is influenza, usually characterised by fever, myalgia, headache and non-productive cough, that may also cause complications with high morbidity and mortality rate, such as pneumonia, myocarditis, central nervous system disease and death [10,11]. In addition, other previously known human coronaviruses cause similar, although milder clinical signs, including the alphacoronaviruses 229E and NL63, and the betacoronaviruses OC43 and HKU1, while two other coronaviruses, SARS-CoV and MERS-CoV, cause severe respiratory syndrome in humans [12].”
Diagnostic algorithm
“The diagnostic algorithm adopted by the Laboratory for SARS-CoV-2 testing included, immediately upon sample receipt, a rapid molecular test for the most common respiratory pathogens in order to obtain a fast differential diagnosis. SARS-CoV-2 testing was based on the protocol released by the World Health Organization (WHO) [13], and three positive patients have been identified at the time of writing this paper.”
Discussion
“Our results highlight the importance of differential diagnosis in travellers arriving from countries with widespread occurrence of COVID-19, considering the similarity of symptoms shared with more common respiratory infections, such as influenza and other respiratory tract diseases.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7055037/
We can see that clinical diagnosis based on symptoms alone is impossible. The only way to differentiate between “viruses” is by the reliance on fraudulent PCR to differentially diagnose “Covid” from other diseases. However, this creates another problem which I have spoken about many times before. In order for the results of the PCR test to be considered accurate, disease prevalence must be known. As defined by the CDC, prevalence is “the proportion of persons in a population who have a particular disease or attribute at a specified point in time or over a specified period of time.” This is how the CDC calculates disease prevalence:
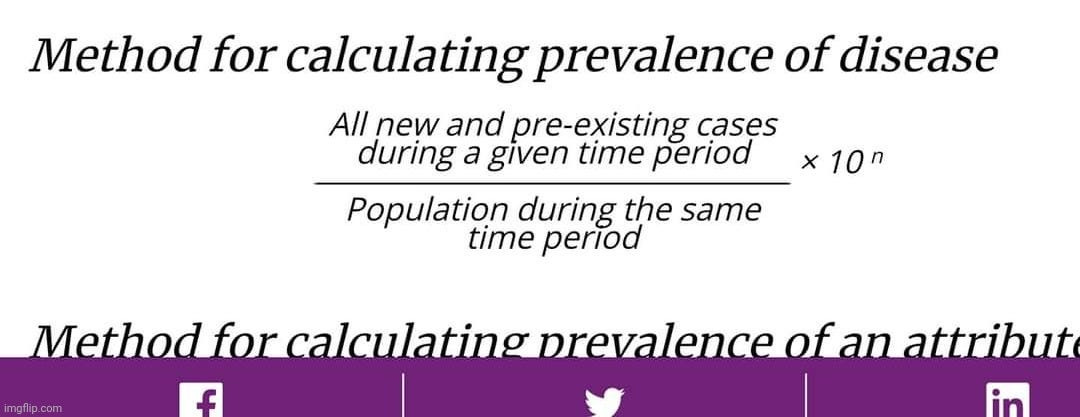
In order to determine prevalence, cases must be known and must come from diagnosis based on clinical symptoms alone. However, as we have discussed, the symptoms are identical between “Covid-19” and many other diseases meaning there is no way to diagnose a patient clinically in order to differentiate cases and thus there is no way to determine disease prevalence. Without knowing disease prevalence, there is no way to determine whether or not any of the test results are being interpreted accurately. This means that all diagnoses, whether clinical or molecular, are false as there is no way to accurately differentiate between “viruses” and the symptoms they are said to cause. For more on the prevalence problem, please see this article.
To further highlight the inability to distinguish between “viruses” clinically in order to determine cases so that disease prevalence can be established, a September 2021 study attempting to create a differential diagnosis between “Covid” and other diseases stated that “Covid” can not be differentiated from other respiratory infections via clinical signs, symptoms, or laboratory results. It was once again reiterated that the symptoms were non-specific and overlapped with many other conditions. The researchers stated that establishing differential diagnosis criteria remained very challenging and that clinical discrimination was unreliable as there were no clinical or laboratory parameters that could be relied upon:
What about the others: differential diagnosis of COVID-19 in a German emergency department
“For many common ED diagnoses, COVID-19 should be considered a differential diagnosis. COVID-19 cannot be distinguished from COVID-19 negative respiratory infections by clinical signs, symptoms, or laboratory results. When hospitalization is necessary, the clinical course of COVID-19 airway infections seems to be more severe compared to other respiratory infections.”
“Most patients with mild symptoms can be treated as outpatients, whereas severely ill COVID-19 patients and patients with similar symptoms cross their way in the emergency department (ED). The variety of symptoms is broad and therefore challenging during primary triage, especially to avoid further spread of the infection and to protect staff from infection.
A report of over 370,000 documented symptomatic cases in the U.S. found cough (50%), fever (43%), myalgia (36%), headache (34%), and dyspnea (29%) to be the most common symptoms, but diarrhea (19%), nausea (12%) and taste/smell disorders (< 10%) were also present in a relevant number of cases [11]. Many of these can be found in other common ED diagnoses comprising heart failure, acute coronary syndrome, exacerbation of COPD, and even gastroenterological and oncological diagnoses. Older patients may present with an atypical and therefore misleading clinical picture consisting of falls and malaise [12].
However, a clinical differential diagnosis between COVID-19 and patients presenting with similar symptoms would be very helpful during primary triage.”
Discussion
“Early triage and differential diagnosis of patients presenting with typical clinical symptoms of COVID-19 remain very challenging but relevant. Our study had the following main findings:
- Differential diagnosis of typical COVID-19 symptoms is very broad and comprises many common respiratory, infectious, and cardiovascular diseases, whereas respiratory diseases are the most frequent. Diseases from nearly every field of clinical medicine can mimic a clinical picture like that of COVID-19, with respiratory diseases being the most prevalent. Older patients may be even more challenging since the clinical picture may be atypical with syncope and malaise [12].
- Patients with COVID-19 present with similar symptoms as COVID-19 negative respiratory infections, so clinical discrimination is not reliable.”
Conclusions
“Differential diagnoses of COVID-19 are plentiful and comprise many common diseases, most notably ailments associated with respiratory impairment. Triage remains challenging in the emergency department since there are no reliable clinical or laboratory parameters to distinguish safely between COVID-19 and airway infections of other origins. When inpatient, COVID-19 takes a more severe clinical course than comparable COVID-19 negative airway infections. Therefore, a strict isolation policy together with broad and rapid testing will remain the most important measures for the months to come.”
https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-021-06663-x
In a May 2022 Cochrane review, the author concluded that symptoms have poor diagnostic accuracy and can not rule in or out disease. While the author resorted to the false uniqueness of anosmia and a cough as possible red flags for “Covid,” this was in regards to using fraudulent molecular tests to rule in or out whether the symptoms were caused by “SARS-COV-2,” not that these symptoms themselves were able to be used to diagnose “Covid” clinically. It was also stated that there is no evidence to support further testing with PCR in any individuals presenting only with upper respiratory symptoms such as sore throat, coryza or rhinorrhoea. It was concluded that the diagnostic accuracy of symptoms for “COVID-19” was moderate to low and could only be used to determine whether or not to test. In other words, the test result is the diagnosis, not the presenting symptoms:
How accurate are symptoms and medical examination to diagnose COVID-19?
“Most individual symptoms included in this review have poor diagnostic accuracy. Neither absence nor presence of symptoms are accurate enough to rule in or rule out the disease. The presence of anosmia or ageusia may be useful as a red flag for the presence of COVID-19. The presence of cough also supports further testing. There is currently no evidence to support further testing with PCR in any individuals presenting only with upper respiratory symptoms such as sore throat, coryza or rhinorrhoea.
Combinations of symptoms with other readily available information such as contact or travel history, or the local recent case detection rate may prove more useful and should be further investigated in an unselected population presenting to primary care or hospital outpatient settings.
The diagnostic accuracy of symptoms for COVID-19 is moderate to low and any testing strategy using symptoms as selection mechanism will result in both large numbers of missed cases and large numbers of people requiring testing. Which one of these is minimised, is determined by the goal of COVID-19 testing strategies, that is, controlling the epidemic by isolating every possible case versus identifying those with clinically important disease so that they can be monitored or treated to optimise their prognosis. The former will require a testing strategy that uses very few symptoms as entry criterion for testing, the latter could focus on more specific symptoms such as fever and anosmia.”

In order to put a final nail in the claim that these “viruses” and the resulting diseases can be differentiated and diagnosed clinically, the British Medical Journal (BMJ) provided a list of conditions which should be differentially diagnosed with ‘Covid” based upon the similarities. However, while doing so, they provided the evidence that this was in fact impossible and that negative results from molecular tests were the only means of differentiation, which as we know are fraudulent without being calibrated/validated to purified/isolated “viruses” and without being able to determine disease prevalence clinically:
Community-acquired pneumonia
SIGNS / SYMPTOMS
Differentiating COVID-19 from community-acquired bacterial pneumonia is not usually possible from signs and symptoms.
Influenza infection
SIGNS / SYMPTOMS
Differentiating COVID-19 from community-acquired respiratory tract infections is not possible from signs and symptoms.
Common cold
SIGNS / SYMPTOMS
Differentiating COVID-19 from community-acquired respiratory tract infections is not possible from signs and symptoms.
Other viral or bacterial respiratory infections
SIGNS / SYMPTOMS
Differentiating COVID-19 from community-acquired respiratory tract infections is not possible from signs and symptoms.
Aspiration pneumonia
SIGNS / SYMPTOMS
Differentiating COVID-19 from aspiration pneumonia is not usually possible from signs and symptoms.
Pneumocystis jirovecii pneumonia
SIGNS / SYMPTOMS
Differentiating COVID-19 from pneumocystis jirovecii pneumonia is not usually possible from signs and symptoms.
Middle East respiratory syndrome (MERS)
SIGNS / SYMPTOMS
Travel history to the Middle East or contact with a confirmed case of MERS.
Differentiating COVID-19 from MERS is not possible from signs and symptoms.
Other
SIGNS / SYMPTOMS
COVID-19 should be considered a differential diagnosis for many conditions. The differential is very broad and includes many common respiratory, infectious, cardiovascular, oncologic, and gastrointestinal diseases.[717]
INVESTIGATIONS
RT-PCR: negative for SARS-CoV-2 viral RNA.
Other differentiating tests depend on the suspected diagnosis.
https://bestpractice.bmj.com/topics/en-us/3000168/differentials
It should be clear now that the differential diagnosis of diseases caused by specific “viruses” by way of clinical symptoms is impossible. This is why the phrase “It’s only viral and needs to run its course” became a common occurrence at doctors’ offices. Yet, with the advent of molecular tests, it became a misconception that PCR, NAAT’s, and antibody tests could be used to distinguish between “viruses.” However, the problem remains that not a single one of these tests have ever been calibrated and validated to actual purified and isolated “viral” particles. These tests all rely on disease prevalence to be known in order to be accurate. This was pointed out by the WHO in January 2021:
“WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.“
https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05

As disease prevalence requires cases of a “virus” to be determined by differential diagnosis based on clinical symptoms, which is impossible, this means that all test results are false positives as true disease prevalence can never be known. Nevertheless, this has not stopped the medical cartel from authorizing and promoting these fraudulent tests as definitive diagnostic tools. This is why we are currently embroiled in a Testing Pandemic, not a “viral” one. This can be seen by the way testing is used to manipulate the perception that the same symptoms of disease are different “viruses” rising and falling due to factors other than the increase and decrease of testing priority. For example, it is well known that “SARS-COV-2” was preferentially tested throughout the “pandemic.” Yet in June 2021, the CDC advised for the testing of RSV for any negative “Covid” tests. Thus, instead of the “It’s not Covid, it’s just another virus and it needs to run its course,” it became “If it isn’t Covid, it must be RSV.” As this increased testing has occurred, so too has a rise in RSV cases:
Coronavirus and RSV
“In June 2021, the CDC issued an official “health advisory” about a rise in RSV cases across the southern United States. It recommended that health care providers test for RSV in all people of any age who have signs and symptoms of respiratory illness, but test negative for the coronavirus.”
https://www.webmd.com/lung/covid19-rsv
It is well known that flu (and other respiratory “viruses”) cases declined in 2020 due to decreased testing as there was a lack of testing materials as they were being used to diagnose “Covid.” However, in 2021 medical institutions increased influenza testing on any negative “Covid” test which resulted in increased cases:
Last year vs. this year
“In 2020, public health officials saw unusually low levels of circulating flu being detected.
There are several different reasons for those low levels of flu. Some of them stemmed from significant challenges with testing supplies. Many of the materials needed to create and process COVID tests are the same materials used to create and process flu tests. This wasn’t an issue only in New York or even the U.S.; those shortages were happening worldwide.
Beyond the limited availability of testing materials, other factors that may have played a role in a lower overall number of flu cases include:
- COVID-related lockdowns
- Wearing masks/face coverings in indoor public settings
- Increased hand hygiene
- Increased physical distancing
In 2021, a rise in flu cases has been observed over the last several weeks. The New York State Department of Health is deeming influenza to be widespread – meaning there are multiple cases in more than half of New York counties.
“In terms of diagnostic testing, our labs will screen patients for flu if their COVID test is negative,” Dr. Laguio-Vila said. “We are actively looking for influenza cases when it comes to testing.”
https://hive.rochesterregional.org/2021/12/twindemic-2021
The CDC admitted in two separate studies that a decrease in respiratory “virus” testing contributed to the decrease in flu and other respiratory disease cases at the beginning of the “pandemic.” This was due to preferential testing for “Covid” over everything else. They admitted that if visits were not made to healthcare sites participating in surveillance, this reduced the amount of testing performed and decreased the number of cases. They also stated that testing capabilities change annually as do the intentions of which pathogens are tested for in a given year:
“The findings in this report are subject to at least three limitations. First, changes in health-seeking behaviors during the pandemic (e.g., designated testing sites for COVID-19) might have contributed to a decrease in reported respiratory virus activity if routine health care visits were not made to health care providers who participate in surveillance. Testing for respiratory viruses was somewhat reduced during 2020–2021 but was higher than typically seen during periods of low virus activity”.
“Some influenza clinical laboratory data and all other respiratory virus data are aggregate, weekly numbers of nucleic acid amplification tests and detections reported to NREVSS, a passive, voluntary surveillance network of clinical, commercial, and public health laboratories. NREVSS aggregate, weekly tests are reported specifically for each pathogen. NREVSS participating laboratories’ testing capabilities vary annually, and testing intentions vary for each pathogen. A range of 50–178 laboratories met the pathogen-specific criteria for inclusion criteria during a given surveillance year.”
https://www.cdc.gov/mmwr/volumes/70/wr/mm7029a1.htm
“Data from clinical laboratories in the United States indicated a 61% decrease in the number of specimens submitted (from a median of 49,696 per week during September 29, 2019–February 29, 2020, to 19,537 during March 1–May 16, 2020) and a 98% decrease in influenza activity as measured by percentage of submitted specimens testing positive (from a median of 19.34% to 0.33%).”
“Initially, declines in influenza virus activity were attributed to decreased testing, because persons with respiratory symptoms were often preferentially referred for SARS-CoV-2 assessment and testing.”
https://www.cdc.gov/mmwr/volumes/69/wr/mm6937a6.htm
Even the WHO’s Director General Tedros Adhanom Ghebreyesus admitted that whether cases rise or fall is related to the amount of fraudulent testing performed:
“Perhaps influenza testing fell away as countries concentrated their resources on COVID-19. Large numbers of people might have struggled through bouts of influenza at home, hidden from the statisticians. In a briefing to the media on June 15, 2020, WHO director-general Tedros Adhanom Ghebreyesus noted that “influenza surveillance has either been suspended or is declining in many countries, and there has been a sharp decline in sharing of influenza information and viruses because of the COVID-19 pandemic”. He added that “compared with the last 3 years, we’ve seen a dramatic decrease in the number of specimens tested for influenza globally”.
https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30508-7/fulltext

Thus, we can clearly see that differentiating between different “viruses” has absolutely nothing to do with clinical diagnosis, which is considered impossible. The diagnosis comes from fraudulent molecular testing, which can never be accurate as the tests were never calibrated nor validated to the assumed “viral” particles in the first place. As test accuracy also relies upon disease prevalence to be determined clinically prior to testing, the results will always be false, and a misdiagnosis will always occur. As long as the medical institutions continue to play the foolish game of trying to differentiate between the various stages of same symptoms of the same detoxification process in order to provide chemical toxins as a “cure,” there can be no progress towards understanding how to truly heal in a time of dis-ease.
This article originally appeared on ViroLIEgy’s Antiviral Substack.
4 Responses
gf7777
Here is another example of fraudulent testing.
Muslims and Jews Finally Agree on Something to Cause a Ceasefire in Gaza: Mass Vaccine Campaign Against Children in Fake Polio Outbreak
“Hamas and Israeli forces have finally found mutual ground to order a ceasefire in the Gaza strip: a mass vaccination campaign against children to force them to receive the deadly oral polio vaccine that is banned in most Western countries, for a fake polio outbreak that is admittedly based on evidence of vaccine-induced polio found in sewage samples.”
https://vaccineimpact.com/2024/muslims-and-jews-finally-agree-on-something-to-cause-a-cease-fire-in-gaza-mass-vaccine-campaign-against-children-in-fake-polio-outbreak/
gf7777
A little off topic but interesting nonetheless – the transcript of a conversation with Copilot.
Sent by you:
was Harold Hillman ever proven wrong?
Sent by Copilot:
Harold Hillman, a British neurophysiologist, was known for his controversial views on cell structure and electron microscopy. He argued that many structures observed under electron microscopes were artifacts created by the preparation process, and he questioned the validity of widely accepted cell structures.
While Hillman’s views were not widely accepted by the scientific community, they were never definitively proven wrong. Instead, his ideas were largely dismissed because they contradicted a substantial body of evidence from various microscopy techniques. Hillman’s insistence on his theories led to professional isolation and ultimately impacted his career.
Sent by you:
if the current model of the cell is wrong what does that mean for virology?
Sent by Copilot:
If the current model of the cell were proven to be incorrect, it would have significant implications for virology and many other fields of biology. Here are some potential impacts:
Virus-Host Interactions: Our understanding of how viruses interact with host cells is based on the current cell model. If this model is wrong, it could mean that the mechanisms of viral entry, replication, and egress are different from what we currently believe.
Diagnostic Methods: Many diagnostic tests for viral infections rely on our understanding of cell biology. For example, PCR tests depend on the knowledge of cellular nucleic acids. A shift in the cell model could necessitate the development of new diagnostic techniques.
Vaccine Development: Vaccines are designed based on how viruses interact with cells and the immune system. An incorrect cell model could lead to ineffective vaccines or require new strategies for vaccine development.
Antiviral Therapies: Current antiviral drugs target specific stages of the viral life cycle within the host cell. If our understanding of these stages is flawed, it could mean that existing drugs are less effective than we think, and new drugs would need to be developed.
Research and Experimental Models: Much of virology research relies on cell culture models. If the cell model is incorrect, it could invalidate many experimental results and require a re-evaluation of past studies.
Educational and Theoretical Frameworks: Textbooks and educational materials would need to be revised, and theoretical frameworks in virology and cell biology would need to be updated to reflect the new understanding6.
Overall, while such a paradigm shift would be challenging, it could also lead to new discoveries and advancements in virology and related fields.
Sent by you:
does electron microscopy produce artifacts?
Sent by Copilot:
Yes, electron microscopy can produce artifacts. Artifacts are distortions or errors in images that do not accurately represent the sample’s true structure or composition. These discrepancies can occur due to various reasons during sample preparation, imaging, or even due to the intrinsic properties of the materials being analyzed.
Here are some common sources of artifacts in electron microscopy:
Sample Preparation: Mechanical, chemical, ionic, or physical actions during sample preparation can introduce artifacts. For example, mechanical polishing or chemical fixation can alter the sample’s structure.
Irradiation: During observation, especially in Transmission Electron Microscopy (TEM), artifacts can be produced due to irradiation under the electron beam. This can cause thermal effects or electronic irradiation damage.
Imaging Conditions: Factors like improper settings, contamination, or charging effects can also lead to artifacts.
Sent by you:
how much damage does an electron beam do to a living cell?
Sent by Copilot:
Electron beams can cause significant damage to living cells. The high-energy electrons used in electron microscopy can break chemical bonds and generate reactive chemical species, leading to structural damage. Here are some specific effects:
Radiation Damage: The electron beam can cause the breakdown of molecular bonds, leading to the formation of free radicals and other reactive species that can damage cellular components.
Desiccation: The vacuum conditions required for electron microscopy can cause rapid evaporation of water from cells, leading to their collapse and death.
Thermal Effects: The energy from the electron beam can also cause localized heating, which can further damage cellular structures.
Due to these effects, electron microscopy is typically not used for imaging living cells. Instead, cells are often fixed, dehydrated, and coated with a conductive material to withstand the electron beam. However, some advanced techniques, like cryo-electron microscopy, aim to minimize these damages by imaging cells at very low temperatures.
Sent by you:
can cryo-electron microscopy produce artifacts?
Sent by Copilot:
Yes, cryo-electron microscopy (cryo-EM) can produce artifacts, although it generally preserves the native structure of samples better than traditional electron microscopy. Here are some common sources of artifacts in cryo-EM:
Ice Crystal Formation: If the sample is not vitrified properly, ice crystals can form, which can distort the sample’s structure.
Beam-Induced Damage: Even at cryogenic temperatures, the electron beam can still cause some damage to the sample, leading to artifacts.
Sample Preparation: Artifacts can also arise during the preparation process, such as during the thinning of samples or the application of cryoprotectants.
Despite these potential issues, cryo-EM is highly valued for its ability to provide near-atomic resolution images of biological molecules and complexes while minimizing many of the artifacts associated with other electron microscopy techniques.
Sent by you:
can the components of the human cell be seen under a light microscope?
Sent by Copilot:
Yes, some components of human cells can be seen under a light microscope, but there are limitations. Here are a few key points:
Visible Components: The nucleus, cell membrane, and sometimes the nucleolus can be seen clearly with a light microscope. These structures are relatively large and can be distinguished with basic staining techniques.
Organelles: Some larger organelles like mitochondria and the Golgi apparatus might be visible, but they often require special stains to be seen clearly. Other smaller organelles, such as ribosomes, are too small to be resolved by light microscopy.
Staining: To see more details, cells are often stained with dyes that bind to specific cell components. This helps to highlight structures that would otherwise be transparent.
Limitations: The resolving power of a light microscope is limited to about 200 nanometers, which means it can’t resolve structures smaller than this. For more detailed views of smaller organelles, electron microscopy is used.
Sent by you:
does electron microscopy show living cells in action?
Sent by Copilot:
Electron microscopy, particularly traditional methods like transmission electron microscopy (TEM) and scanning electron microscopy (SEM), cannot show living cells in action because the samples must be placed in a vacuum and often require extensive preparation, including fixation and dehydration, which kills the cells.
However, advancements in techniques like cryo-electron microscopy (cryo-EM) and time-resolved cryo-EM are pushing the boundaries. Cryo-EM involves rapidly freezing cells to capture their structures in a near-native state, allowing researchers to see detailed images of cellular components. Time-resolved cryo-EM can capture molecular processes in action by taking snapshots at different time points, creating a sort of “movie” of molecular events.
While these methods provide incredible detail and insights into cellular processes, they still don’t show living cells in real-time action. For real-time imaging of living cells, techniques like fluorescence microscopy and live-cell imaging are more suitable.
Sent by you:
how accurate is fluorescence microscopy?
Sent by Copilot:
Fluorescence microscopy is a powerful tool for visualizing and quantifying biological specimens, but its accuracy can be influenced by several factors:
Resolution: Fluorescence microscopy can achieve high spatial resolution, especially with techniques like confocal microscopy and super-resolution microscopy (e.g., STED, PALM/STORM). However, the resolution is still limited by the diffraction limit of light, typically around 200 nanometers.
Quantitative Accuracy: The accuracy of quantitative measurements in fluorescence microscopy depends on the proper calibration of the imaging system and the use of appropriate controls. Errors can arise from the specimen, the microscope, or the detector. For example, photobleaching (loss of fluorescence over time) and phototoxicity (damage to the specimen from light exposure) can affect accuracy.
Fluorophore Properties: The choice of fluorophores and their photophysical properties (e.g., brightness, photostability) also impact accuracy. Fluorophores with high quantum yield and stability provide more reliable results.
Image Analysis: Accurate image analysis requires sophisticated software and algorithms to quantify fluorescence intensity and spatial distribution. Errors in image processing can lead to inaccuracies.
Environmental Factors: Temperature, pH, and other environmental conditions can affect fluorescence signals. Maintaining consistent conditions during experiments is crucial for accuracy.
Overall, while fluorescence microscopy is highly accurate for many applications, careful experimental design and proper controls are essential to minimize errors and ensure reliable results.
Sent by you:
is bioinformatics used in fluorescence microscopy?
Sent by Copilot:
Yes, bioinformatics is increasingly used in fluorescence microscopy, particularly in the analysis and interpretation of complex data. Here are some key areas where bioinformatics plays a role:
Image Analysis: Bioinformatics tools and algorithms are used to process and analyze fluorescence microscopy images. This includes tasks like segmentation (identifying and separating different parts of the image), quantification of fluorescence intensity, and tracking of fluorescently labeled molecules or cells over time.
Super-Resolution Microscopy: Techniques like single-molecule localization microscopy (SMLM) generate large datasets that require sophisticated computational methods for accurate reconstruction of images. Bioinformatics approaches, including deep learning and Bayesian inference, are used to enhance the resolution and accuracy of these images.
Data Integration: Bioinformatics helps integrate fluorescence microscopy data with other types of biological data, such as genomic, proteomic, and transcriptomic data. This integration can provide a more comprehensive understanding of cellular processes and functions.
Automated Classification: Machine learning algorithms, a subset of bioinformatics, are used to automatically classify subcellular structures and patterns in fluorescence microscopy images. This can significantly speed up the analysis process and improve accuracy.
Simulation and Modeling: Bioinformatics tools are used to simulate and model biological processes observed under fluorescence microscopy. This can help in understanding the dynamics of these processes and predicting their behavior under different conditions.
These applications demonstrate how bioinformatics enhances the capabilities of fluorescence microscopy, making it a more powerful tool for biological research.
Sent by you:
what are the problems with bioinformatics?
Sent by Copilot:
Bioinformatics is a rapidly evolving field, but it faces several significant challenges:
Data Management: The sheer volume of data generated by modern sequencing technologies is overwhelming. Managing, storing, and retrieving this data efficiently requires substantial computational resources and sophisticated data management systems.
Data Integration: Integrating diverse types of biological data (e.g., genomic, proteomic, transcriptomic) is complex. Different data formats and standards can make it difficult to combine datasets in a meaningful way.
Data Quality and Standardization: Ensuring the quality and consistency of data is a major issue. Variability in data collection methods and lack of standardized formats can lead to errors and inconsistencies.
Computational Resources: High-performance computing resources are essential for processing large-scale bioinformatics data. However, not all research institutions have access to the necessary infrastructure, which can limit the scope of their analyses.
Interpreting Results: Translating raw data into meaningful biological insights is challenging. Bioinformaticians must develop and apply complex algorithms and models to interpret the functional impacts of genomic variations and other data.
Security and Privacy: Protecting sensitive biological data, especially in the context of personalized medicine, is crucial. Ensuring data security and patient privacy while enabling data sharing for research purposes is a delicate balance.
Skill Gaps: There is a growing need for bioinformaticians with expertise in both biology and computational sciences. Bridging this skill gap requires interdisciplinary training and education.
Addressing these challenges requires ongoing collaboration between biologists, computer scientists, and data analysts.
Sent by you:
if the nature of the human cell is based on structured water and ribosomes do not exist what does this mean for virology
Sent by Copilot:
If the nature of human cells were based on structured water and ribosomes did not exist, it would fundamentally alter our understanding of virology and cellular biology. Here are some key implications:
Protein Synthesis: Ribosomes are essential for translating mRNA into proteins. Without ribosomes, an alternative mechanism for protein synthesis would need to exist. This would challenge our current understanding of how viruses hijack host machinery to produce viral proteins.
Viral Replication: Viruses rely on the host cell’s ribosomes to replicate. Without ribosomes, viruses would need to find another way to produce the proteins necessary for their replication and assembly.
Cellular Function: Structured water is thought to play a role in cellular processes, but it does not replace the need for proteins. If cells were primarily based on structured water, it would imply a different mechanism for maintaining cellular functions and integrity.
Antiviral Strategies: Current antiviral drugs often target the interaction between viral components and ribosomes. Without ribosomes, these strategies would be ineffective, necessitating new approaches to antiviral therapy.
Scientific Paradigm Shift: This would represent a significant shift in the scientific paradigm, requiring a reevaluation of many established concepts in molecular biology and virology.
This hypothetical scenario would require a complete rethinking of how we understand both cellular and viral biology. It’s a fascinating thought experiment that highlights the complexity and interdependence of biological systems.
Sent by you:
does x-ray crystallography produce artifacts?
Sent by Copilot:
Yes, X-ray crystallography can produce artifacts, which are misleading features in the data that do not represent the true structure of the molecule being studied. Some common artifacts include:
Radiation Damage: X-rays can damage the crystal, leading to changes in the structure during data collection.
Phase Problem: Errors in phase determination can lead to incorrect electron density maps.
Crystallization Artifacts: Conditions used to grow crystals can sometimes induce non-native conformations or interactions.
Libration Effects: These can cause bond lengths to appear shorter than they actually are.
Inaccurate Hydrogen Positions: Hydrogen atoms are difficult to locate accurately due to their low electron density.
Spurious Features: These can appear in electron density maps, especially near heavy atoms.
Despite these challenges, careful experimental design and data analysis can minimize the impact of artifacts, making X-ray crystallography a powerful tool for determining molecular structures.
Sent by you:
on a percentage basis how accurate is the current model of the living cell?
Sent by Copilot:
The accuracy of the current model of the living cell is generally considered to be quite high, but it is difficult to quantify this accuracy as a specific percentage. The model is based on extensive research and observations using various advanced techniques, including electron microscopy, X-ray crystallography, and molecular biology methods.
However, there are still areas where our understanding is incomplete or evolving. For example:
Complexity of Interactions: The interactions between different cellular components are highly complex and not fully understood. This includes protein-protein interactions, signaling pathways, and the dynamics of cellular processes.
Dynamic Nature: Cells are dynamic systems that constantly change in response to their environment. Capturing this dynamic nature in a static model is challenging.
Technological Limitations: While techniques like electron microscopy and X-ray crystallography provide detailed images, they also have limitations and can introduce artifacts.
Emerging Discoveries: New discoveries, such as the roles of non-coding RNAs and the detailed mechanisms of cellular processes, continually refine and sometimes challenge existing models.
Overall, while the current model of the living cell is highly accurate and reliable for many applications, it is continually being refined and updated as new discoveries are made.
End of conversation.
Mike Stone
Thanks for sharing! That is great info. 🙂
gf7777
I shouldn’t be asking these questions. If these people were real scientists they would be asking these questions. It is the business of a real scientist to try to prove hypotheses and theories wrong. But they don’t do it. They just make up templates and models and align the data to fit it. The problem is the data never comes directly from anything that is unaltered. This is what they present as science today.
Here’s an example of how they abuse science to make money:
Lysol to Donate Minilabs Science Kits to K–12 Schools
“. . . According to the news release, the kits contain educational materials, lesson plans, and classroom activities for teachers. The contents of each kit will vary and revolve around a dedicated theme, like “Germs in the Classroom.”
https://spaces4learning.com/Articles/2024/07/30/Lysol-Donates-Minilabs-Science-Kits.aspx
What a joke.