

Fictional Fear
What we fear, we manifest.
Around this time of the year, I like to highlight a factor in disease that is very often overlooked: the fear factor. Fear—along with its close relatives, anxiety and stress—is well documented to negatively impact physical health. Yet, when discussing illness, people often ignore how profoundly these mental states can mimic or exacerbate disease. The body responds to fear just as it would to the fictional threat of supposed “viruses.”
For instance, in the late nineteenth century, Louis Pasteur, the very father of germ “theory,” inadvertently documented the power of fear and its close connection to so-called “viral” disease. In defending his rabies vaccine after deaths were attributed to it, he invoked what he called “false rabies.” In one case, a man developed classic rabies symptoms—including throat spasms, chest pain, and extreme anxiety—merely after a lunchtime discussion about the disease, despite never having encountered a rabid animal. In another, a magistrate became delirious and developed a horror of water after learning that a dog that had licked his hand long before was suspected of rabies. His symptoms disappeared only after his physician assured him he would already be dead if he had “true rabies.”
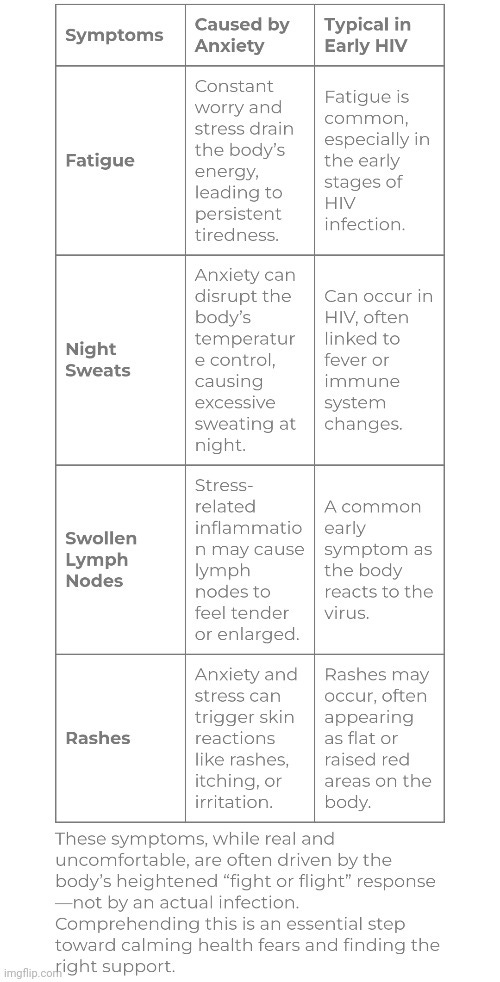
This same phenomenon persists today. A condition known as HIV phobia illustrates how fear alone can produce symptoms indistinguishable from those attributed to “infection.” Those suffering from HIV phobia experience real physical effects, including fatigue, night sweats, rashes, and swollen lymph nodes, all driven entirely by anxiety rather than any “virus.” Despite repeated negative tests, many remain convinced they are ill. Even mainstream sources acknowledge that the cause is psychological, not microbial—rooted in misinformation, stigma, and fear.
Modern research repeatedly confirms that fear, stress, and anxiety can produce physical symptoms identical to those attributed to “viral” disease. In the UK, people with severe “Covid” anxiety reported more than double the rate of somatic symptoms (chest pain, dizziness, palpitations) after the “pandemic” than before—despite many having no new health problems.
A systematic review of 36 studies found that in all segments of society (healthcare workers, the general public), symptoms like shortness of breath, joint/muscle pain, palpitations and more were highly prevalent during the “pandemic,” often in people without “confirmed infection,” and strongly associated with anxiety, stress, and depression.
Even in children and adolescents recovering from “Covid,” studies show that fatigue, emotional distress, and gastrointestinal symptoms are common, correlating with anxiety and mood symptoms more than with the severity of “infection.”
Similar findings appear in fibromyalgia and chronic pain research which confirm that traumatic life events and ongoing stress amplify physical symptoms like fatigue, pain, and malaise in the absence of new “pathogens.”
A 2022 article titled Is Anxiety Making You Feel Sick & Ill? explains how anxiety can cause nausea, breathlessness, dizziness, fatigue, and even flu-like symptoms. Scientists attribute this to activation of the fight-or-flight response, stress hormones like cortisol, and tension affecting the stomach and gut:
Feeling Ill from Anxiety?
You may be coming down with a cold. You may be coming down with a serious disease. Or you may just have anxiety. It’s sometimes hard for people to believe that feeling ill can come from anxiety, but it’s a very real experience that affects many people.
Anxiety Can Cause Feelings of Illness
The stress from anxiety can cause feelings of genuine sickness. These feelings are often very similar to the way physical illnesses make you feel. Your stomach can feel like it’s rumbling and you may even feel nauseated. Feeling sick may be a sign that you’ve fallen ill, but it can also be a sign of anxiety.
While feeling sick may be the only physical symptom of anxiety, there are often others including breathlessness, dizziness and fatigue.
Why Does Anxiety Cause a Sick Feeling?
In general, that sick feeling is caused by a number of different factors. Just a few of which include:
- Standard Stress Response: Scientists believe that nausea, and some of the common feelings of illness, are the result of issues with related to the activation of the fight or flight response and the hormones related to stress, like cortisol.
- Gut and Abdominal Pressure: Anxiety can also lead to increased muscle tension that causes pressure on the stomach and guts. It is possible that this pressure affects how your stomach feels and thus gives you a sick feeling.
- Mild Illness: Your body fights off germs every day. Anxiety can weaken your immune system, increasing the risk of developing common minor illnesses. This may also contribute to a feeling of nausea and sickness.
Feeling ill is something that often causes concern. Some people feel so sick that they vomit or experience profound nausea that keeps them away from their activities. In this way, the physical effects of anxiety can cause further anxiety, creating a cycle.
Some people experience more than just nausea when anxious. They may experience other symptoms that are similar to catching a cold or flu. They may feel like their glands are swollen, or their tongue is dry. They may feel lightheaded. They may even cough or experience severe stomach discomfort, like indigestion.
These psychosomatic effects blur the line between emotional distress and physical illness. A racing heart, shallow breathing, chest tightness, feverish sensations can all be misinterpreted as signs of “infection.” Once a person believes they have “caught” something, the fear amplifies the symptoms further, locking them into a feedback loop of anxiety and physiological response. The mind and body become the perfect incubator—not for a “virus,” but for fear itself.
This is closely related to what scientists call the nocebo effect—the opposite of the placebo effect—where negative expectations and fear cause real, measurable harm to the body. Studies have shown that simply believing one is exposed to a “pathogen” or toxin can trigger the same symptoms as actual exposure.
Once we understand how easily fear alone can generate the appearance of illness, it becomes clear why it has been such an effective tool for control. Fear works. And those in power know it. Scary images of people collapsing in the street. Alarming headlines about an invisible threat ready to attack the “unprotected.” A running death counter on every screen. Lockdowns, quarantines, masks, and constant sanitizing. Even mild, ordinary symptoms, like loss of taste or smell, suddenly amplified through fear. Add a fraudulent test that counts the healthy among the “infected,” and you have the perfect recipe for a “pandemic” of fear.
To illustrate how this dynamic plays out, here is an excellent short video from Universe Simple that imagines an alternate timeline where fear itself is treated as a literal “virus.”
Fear fills the gaps where understanding is absent. When people do not know why they are sick, fear rushes in to offer an answer, and it is one that is easy to control, label, and sell. This psychological vulnerability has been exploited for over a century under the guise of “germ science.”
I wrote a very in-depth article on this very subject back in 2022, and I added an addendum to it in 2024. The full article, titled Fear is the Real “Virus,” contains far more details and evidence demonstrating how fear is weaponized against us. To help spread this overlooked truth, I also recently designed T-shirts with this very message, available in the ViroLIEgy Shop:

Fictional Fear T-shirt (Regular Edition)

Fictional Fear T-shirt (Halloween Edition)
A big part of exposing the fraud of germ “theory” and virology is highlighting and educating people on well-documented, alternative factors in disease that need no invisible “pathogen” as a scapegoat. Fear and anxiety are not fringe ideas. They are proven stressors that can mirror or even drive illness. Yet these common-sense realities have been sidelined in favor of a perpetual war on invisible invaders. The real weapon is not a microbe—it is fear itself. And the only true immunity comes from breaking its hold through understanding the fraud of germ “theory” and virology.
2 Responses
Shirley
I totally agree with this! I work in a health food store, but rarely watch/listen to the news. At the very beginning of the pandemic I had vaguely heard about it, and didn’t think much about it. Then all of a sudden we had people coming in the store absolutely terrified! And I’m thinking there’s something wrong with this picture, that so much fear was being generated. I knew right away this so called pandemic was not real! It was a pandemic of fear!
gf7777
Great article Mike. I witnessed the fear and its consequences during the scamdemic, and it is very real. People are definitely affected by fear. I was wondering if you know anything about kidney disease. My wife’s doctor keeps testing her for particle concentrations. And it kind of reminds me of the PCR test to some degree. I compiled a brief article. It’s just speculative at this point. I’d like to get some opinions on it.
The Diagnostic Mirage: Rethinking Chronic Kidney Disease Through Terrain Logic and Institutional Audit
Chronic Kidney Disease (CKD) is widely recognized as a progressive condition affecting millions worldwide. Yet beneath its clinical veneer lies a diagnostic architecture riddled with epistemic drift, pharmacological distortion, and institutional inertia. This article audits the procedures, assumptions, and staging logic that define CKD—and asks whether the condition, as currently diagnosed, even exists in the form we’re told.
The Diagnostic Framework: Particle Proxies Over Terrain
CKD is staged using two primary biochemical markers: the Estimated Glomerular Filtration Rate (eGFR), which is derived from serum creatinine using the CKD-EPI equation, and the Urine Albumin-to-Creatinine Ratio (uACR), which measures protein leakage and is interpreted as glomerular damage. These markers are interpreted through KDIGO guidelines, which define CKD as an eGFR below 60 or a uACR above 30 mg/g for a duration of three months or more. However, these thresholds are age-insensitive, terrain-excluded, and pharmacologically vulnerable.
Medication-Induced Distortion: Simulating Disease
Many medications prescribed for unrelated conditions can alter kidney-related particle concentrations, thereby mimicking CKD. For example, NSAIDs reduce renal perfusion and increase creatinine levels. Proton pump inhibitors (PPIs) can cause interstitial nephritis, also leading to elevated creatinine. Diuretics may induce volume depletion, resulting in increased uric acid and decreased GFR. Antibiotics, particularly nephrotoxic ones, can damage tubules and raise creatinine. Antacids may cause calcium overload and nephrocalcinosis. Lithium is known to induce chronic nephropathy and reduce GFR. These effects are rarely modeled before diagnosis, meaning healthy individuals may be staged as diseased due to medication artifacts.
Protocol vs. Physician Autonomy
Physicians are expected to follow standardized CKD protocols. They must use eGFR and uACR thresholds, stage disease based on KDIGO guidelines, and initiate treatment—such as ACE inhibitors or SGLT2 inhibitors—based on lab values rather than symptoms. Deviation from these protocols is discouraged. Alternative diagnostics, such as inulin clearance, hydration challenge, or terrain audit, are not reimbursed or supported. This reduces physicians to technocratic interpreters of lab data, sidelining clinical judgment and patient agency.
Biopsy and Autopsy: Morphology Without Terrain
Biopsies are rarely used in CKD staging. When performed, they sample less than 0.01% of kidney tissue, evaluate dead, fixed tissue in vitro, and cannot model filtration, perfusion, or systemic compensation. Autopsies reveal renal lesions in many undiagnosed individuals, but also show that morphological findings often fail to correlate with symptoms or functional decline. Both biopsy and autopsy treat structure as pathology, ignoring terrain.
Counterfactual Modeling: Treatment vs. Natural Death
In older adults, CKD diagnosis often does not alter outcomes. For example, among individuals aged 65 to 69 diagnosed with CKD Stage 3a, the five-year risk of kidney failure is approximately 0.12%, while the five-year risk of death is around 8 to 10%. For those aged 75 to 79, the kidney failure risk remains at 0.12%, but the death risk rises to 20 to 25%. In individuals aged 80 and above, the kidney failure risk is still 0.12%, while the death risk climbs to 30 to 40%. Death from natural causes vastly exceeds kidney failure risk. Many patients follow the same trajectory with or without diagnosis or treatment.
Terrain Tolerance vs. Protocol Thresholds
The system assumes that elevated particle concentrations—such as creatinine or albuminuria—are direct evidence of organ pathology. But this ignores a critical possibility: what if the terrain, left undisturbed, would recalibrate and stabilize at a higher threshold of particle concentrations without collapse? This isn’t a return to “normal.” It’s a new equilibrium, shaped by the body’s adaptive capacity in the presence of chronic medication layering. And yet, the system never tests this. Once treatment begins, the terrain is altered, and the altered particle concentrations are used to justify continued diagnosis and intervention.
Furthermore, the treatment itself is designed to filter out excess concentrations, assuming that the organ was failing to do so. But this assumption may be flawed. The organ may never have had the opportunity to perform that function—because it was never designed to operate under the altered terrain created by chronic medication use. The accumulation of particles may not reflect malfunction, but rather terrain-induced saturation. This means the system may be sowing the disease with one hand—via medications that distort terrain—and offering the cure with the other, based on the very distortions it created. The terrain becomes pharmacologically saturated. Particle concentrations shift—not due to disease, but due to medication-induced distortion. And these shifts are then diagnosed as CKD. The system never asks whether the terrain would stabilize on its own. It never models adaptive thresholds. It never pauses to observe. This is not just a diagnostic failure—it’s an epistemic collapse.
Falsifiability Gap: No Mechanism to Reverse Diagnosis
Once staged, CKD is rarely re-evaluated. There is no standard protocol to pause medications and re-test. No terrain audit is conducted to assess hydration, nutrition, or stress. No falsifiability logic exists to challenge the diagnosis. This creates a diagnostic loop: particle proxies trigger staging, staging triggers treatment, and treatment reinforces the label.
The Ignored Candidate: Vaccine-Induced Terrain Collapse
Unlike episodic medications or confined exposures, vaccinations are broad-spectrum, demographically synchronized, and repeatedly administered. They bypass all natural defenses—gut, lung, skin—and enter systemic circulation directly. Yet vaccine-related injury is only considered within narrow time windows. For example, anaphylaxis must occur within four hours, Guillain-Barré syndrome within three to forty-two days, and encephalopathy within seventy-two hours. If symptoms emerge outside these windows, they are excluded from causal consideration, even if terrain collapse is evident.
This means cumulative effects from repeated boosters and adjuvants are never modeled. Delayed terrain destabilization is dismissed as idiopathic or age-related. CKD diagnosis may reflect filtration overload, not organ failure—but the most likely candidate is systematically ignored. The diagnostic system is designed to protect the intervention, not interrogate it. And the kidney, as the filtration organ, becomes the scapegoat for systemic bypass.
The Business of CKD
The CKD industry is projected to reach $120.7 billion by 2030. This growth is driven by pharmaceutical sales—including ACE inhibitors, anemia drugs, and SGLT2 inhibitors—alongside dialysis and transplant services, diagnostic labs and imaging, and AI-powered risk tools and wearable monitors. CKD is not just a condition—it’s a multi-billion-dollar architecture, sustained by staging logic and pharmacological layering.
Conclusion: Rethinking CKD Through Terrain Logic
CKD, as currently diagnosed, may reflect medication-induced particle distortion, age-related biochemical drift, protocol-driven overmedicalization, structural findings without functional collapse, systemic bypass from repeated injections, and diagnostic exclusion of the most probable cause. To restore diagnostic integrity, we must reintroduce terrain-integrated logic, demand falsifiability protocols, audit pharmacological and procedural interference, reframe CKD as a constructed condition rather than a deterministic disease, and interrogate the intervention shield that protects systemic bypass from scrutiny.