
“Is this really about the vaccine or is it about something else?”
-Dr. Robert Malone, M.D., M.S. is the discoverer of in-vitro and in-vivo RNA transfection and the inventor of mRNA gene therapy “vaccines,” while he was at the Salk Institute in 1988.
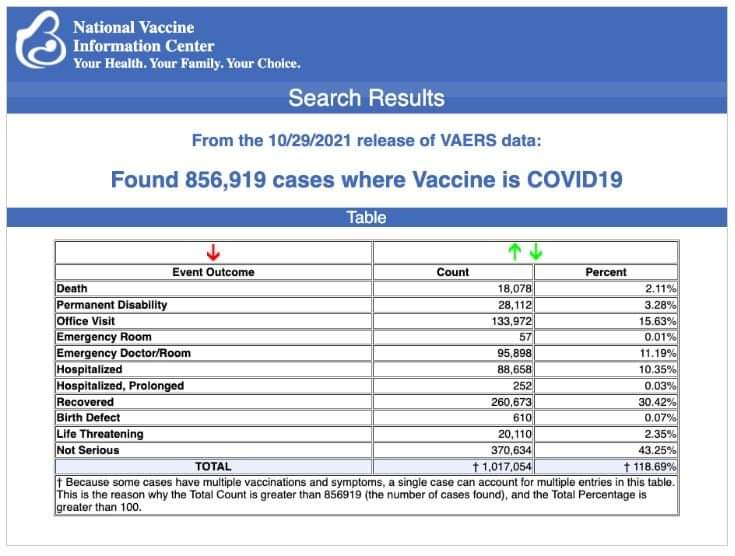
It continues to amaze how, despite the numerous instances of criminality and fraud, people still have faith in the poisons being peddled to them by the pharmaceutical industry. There is plenty of evidence available now about the dangers of various drugs and vaccines that have been pushed to the market with lacking safety data only to be recalled later due to the accumulated reports about the dangerous side effects. There are hundreds of thousands (if not millions) of instances in the VAERS database chronicaling the life-threatening side effects, disabilities, and fatalities suffered by the those who unknowingly subject themselves to a deadly game of pharmaceutical Russian Roulette. There is plenty of information out there on the disastrous state of modern science, with most of the studies being considered inaccurate or false, the inability to reproduce and replicate results, and the inappropriate influence of pharmaceutical money on the scientific journals and the grants handed out to researchers in order to fund the faulty studies.
There are many in the scientific community speaking out about these issues even though there are major efforts to censor and silence them. One man who has been outspoken in his criticism of the scientific institution as well as the potentially deadly consequences of the current mRNA vaccine agenda is the inventor of the mRNA technology himself, Dr. Robeet Malone. Why his message has been allowed to get out is a question that I will not attempt to answer here, but whatever the reason, it is important and his words have value:
“The top federal agencies responsible for public health in the United States, the CDC and the FDA, are “profoundly corrupt” and are forcefully pushing experimental gene therapeutics, aka COVID vaccines, on the population with “grossly incomplete” data that does not meet even the “minimum standards” for safety. Moreover, the vaccination campaign and the other elements of the COVID policies that have been employed by governments worldwide have little to do with the public health at all. So says mRNA vaccine inventor Robert Malone in an exclusive interview with LifeSiteNews.”
There are plenty of other instances of Dr. Malone’s critical appraisal of this current situation we have found ourselves in but I will not list them all here. It is important to understand why a man in such a prominent position in the discovery of the technology currently being hailed as a “miracle cure” against “Covid-19” has become such an outspoken critic. Just as Kary Mullis, inventor of the PCR technique, was adamant about his invention not being used as a diagnostic test, we now have Dr. Malone waving the red flag about the unknown threat of his creation. To see if we can gain some insight into his warnings, let’s see what they “know” as well as what is not known about these mRNA “vaccines.”

What is mRNA?
First, let’s take a look at what mRNA is exactly. According to the National Human Genome Research Institute, mRNA is used to create specific proteins in the body. These molecules are said to put DNA instructions into action:
“Messenger RNA (mRNA) is a single-stranded RNA molecule that is complementary to one of the DNA strands of a gene. The mRNA is an RNA version of the gene that leaves the cell nucleus and moves to the cytoplasm where proteins are made. During protein synthesis, an organelle called a ribosome moves along the mRNA, reads its base sequence, and uses the genetic code to translate each three-base triplet, or codon, into its corresponding amino acid.
Messenger RNAs, also known as mRNA, are one of the types of RNA that are found in the cell. This particular one, like most RNAs, are made in the nucleus and then exported to the cytoplasm where the translation machinery, the machinery that actually makes proteins, binds to these mRNA molecules and reads the code on the mRNA to make a specific protein. So in general, one gene, the DNA for one gene, can be transcribed into an mRNA molecule that will end up making one specific protein.“
https://www.genome.gov/genetics-glossary/messenger-rna

How Do The mRNA Vaccines Work?
To understand how these mRNA vaccines supposedly work, let’s see what both Moderna and the CDC have to say.
From Moderna:
Using mRNA to develop a new category of medicines.
“At Moderna, we are leveraging the fundamental role that mRNA plays in protein synthesis. We have developed proprietary technologies and methods to create mRNA sequences that cells recognize as if they were produced in the body. We focus on diseases where enabling targeted cells to produce – or turn ‘on’ – one or more given proteins will enable the body to fight or prevent a given disease.
- We start with our desired sequence for a protein.
- We design and synthesize the corresponding mRNA sequence – the code that will create that protein.
- Before synthesis, we also engineer that mRNA sequence to optimize the mRNA’s physical properties, as well as those of the encoded protein.
- We deliver the mRNA sequence to the cells responsible for making that protein via one of several modalities. Reaching different types of cells requires different delivery methods.
- And, once the mRNA – the instructions – are in the cell … human biology takes over. Ribosomes read the code and build the protein, and the cells express the protein in the body.
https://www.modernatx.com/mrna-technology/science-and-fundamentals-mrna-technology
From the CDC:
How mRNA Vaccines Work
“To trigger an immune response, many vaccines put a weakened or inactivated germ into our bodies. Not mRNA vaccines. Instead, mRNA vaccines use mRNA created in a laboratory to teach our cells how to make a protein—or even just a piece of a protein—that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies.
1. First, COVID-19 mRNA vaccines are given in the upper arm muscle. The mRNA will enter the muscle cells and instruct the cells’ machinery to produce a harmless piece of what is called the spike protein. The spike protein is found on the surface of the virus that causes COVID-19. After the protein piece is made, our cells break down the mRNA and remove it.
2. Next, our cells display the spike protein piece on their surface. Our immune system recognizes that the protein doesn’t belong there. This triggers our immune system to produce antibodies and activate other immune cells to fight off what it thinks is an infection. This is what your body might do to fight off the infection if you got sick with COVID-19.
3. At the end of the process, our bodies have learned how to protect against future infection from the virus that causes COVID-19. The benefit of COVID-19 mRNA vaccines, like all vaccines, is that those vaccinated gain this protection without ever having to risk the potentially serious consequences of getting sick with COVID-19. Any temporary discomfort experienced after getting the vaccine is a natural part of the process and an indication that the vaccine is working.”
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/mrna.html

According to both Moderna and the CDC, mRNA vaccines work by way of these injectable molecules going directly into the muscle cells which then use the blueprint given by the mRNA to create copies of the desired protein. Once the body creates this protein, it wants to immediately get rid of it as the protein is unrecognizable and doesn’t belong there. This creates the “immune response,” a.k.a inflammation, which is the process the body goes through when healing from unwanted toxins. Of course, they want people to believe that the inflammation created is a good thing and means that the vaccine is working by creating antibodies when in reality, the body has been poisoned by synthetic lab creations injected directly the bloodstream along with various toxins and it is immediately attempting to flush these poisonous chemicals out. Creating an inflammatory response does not equal the body producing an army of theoretical “virus-fighting” antibodies hanging out to protect from any future “virus” infection. This is easily disproven by the lack of antibody results in some of the vaccinated and the still unknown correlation of protection. It is simply a detoxification process.
mRNA Theory
Keep in mind that the function and use of mRNA is purely theoretical. The way the mRNA vaccines work is based on guesswork involving unseen molecules carrying out unseen processes within cells in the body. This is admitted in an article from the Association of American Medical Colleges in March 2021:
mRNA technology promises to revolutionize future vaccines and treatments for cancer, infectious diseases
“The theory behind the vaccines is that mRNA will tell a cell to make a protein that’s used by a certain virus, which would set off an immune response that builds the body’s ability to fend off the actual virus.
“It’s essentially biological software,” Cooke says.
The theory showed promise in lab experiments and animal trials through the 1990s and early 2000s, with researchers aiming to create therapies to stop the spread of cancer and vaccines to protect against such viral diseases as influenza, Ebola, and SARS (severe acute respiratory syndrome).”
“Several stubborn drawbacks impeded the technology’s usefulness: It was difficult to get mRNA into a cell, and mRNA caused severe inflammation and was quickly degraded by the body. In what mRNA researchers consider a breakthrough, Weissman and fellow PSOM researcher Katalin Karikó, PhD, overcame those hurdles by using synthetic RNA that the body’s immune system doesn’t recognize and encasing that material in lipid nanoparticles (fat bubbles) that easily slip into cells.”
Moderna also spoke of this theory back in 2018:
Can mRNA disrupt the drug industry?
“Moderna offered a different proposition: What if instead, mRNA was given therapeutically? In theory, it could prompt proteins to be made in your body. It would put the drug factory inside you.
The idea Hoge was selling is straightforward, but its implementation is not. When mRNA is injected into the body, it triggers virus-detecting immune sensors. That event causes cells to shut down protein production, thus foiling the therapy. And even if the molecule makes it into the cell—another challenge that has long vexed drug delivery experts—the mRNA might not make enough protein to actually be useful.”
“Moderna’s slick storytelling has helped Bancel raise over $1.7 billion—all from private investors—to try to realize his ambitious plan. It has also invited skeptics, who would like to see those ambitions backed up by data.”
“But Moderna has catalyzed an excitement for therapeutic mRNA that is spilling into other start-ups and even big pharma companies. Collectively, they think they have overcome some of the fundamental challenges of translating mRNA from idea to product.”
https://cen.acs.org/business/start-ups/mRNA-disrupt-drug-industry/96/i35
They have sold the public on a theory of how these synthetic lab creations may possibly work as a vaccine inside the body. Their “slick storytelling” mixed with an effective fear-propaganda campaign run by the pharmaceutical-controlled CDC/WHO/FDA/MSM has convinced the ignorant to line up as human Guinea pigs for unproven experimental gene-therapy masquerading as a vaccine. The overwhelming list of adverse reactions and deaths reported to VAERS (estimated to be less than 1% of actual totals) and other sources should cause alarm bells going off in anyone’s head.

Dangerous Ingredients
Besides the synthetic lab-created mRNA itself, what else could be causing such a strong inflammatory response in many individuals receiving these hazardous concoctions? What are the ingredients in these mRNA vaccines? In the image above, you can see what is admitted to the be in the Moderna, Pfizer and even the J&J vaccines. Below is a breakdown of these ingredients in the Moderna vaccine (which is very similar to Pfizer) and a closer look at the potential toxicities for a few of them:
The Moderna COVID-19 Vaccine is made of the following ingredients:
- mRNA – Like the Pfizer BioNTech vaccine, Moderna’s also uses mRNA technology to build antibodies against COVID-19.
- Lipids – The Moderna vaccine also requires lipids to help deliver the mRNA to the cells.
- SM-102
- 1,2-dimyristoyl-rac-glycero3-methoxypolyethylene glycol-2000 [PEG2000-DMG]
- cholesterol
- 1,2-distearoyl-snglycero-3-phosphocholine [DSPC]
The remaining ingredients (below), including acids, acid stabilizers, salt and sugar all work together to maintain the stability of the vaccine after it’s produced.
- Acids
- Acetic acid
- Acid Stabilizers
- Tromethamine & Tromethamine hydrochloride
- Salts
- Sodium acetate
- Sugar
- Sucrose
A Simple Breakdown of the Ingredients in the COVID Vaccines
Lipid Nanoparticles
Lipid nanoparticles are key components of the mRNA vaccines and are said to protect and transport the mRNA to the right places. Like the mRNA, lipid nanoparticles are created synthetically in the lab. They can induce allergic reactions such as anaphylaxis and have been linked to increased white blood cells, changes in coagulation parameters, and liver toxicity among other reactions in rats and monkeys. Nanoparticles themselves are known to be toxic and the safety data is lacking:
Allergic reactions to the mRNA COVID-19 vaccines
“Despite their clear advantages for drug delivery, lipid nanoparticles have an unwanted side-effect; they have the potential to induce an allergic reaction, particularly for those who suffer with severe allergies. However, reactions are rare and researchers estimate a rate of 1.1 cases of anaphylaxis for every million first doses of the Pfizer/BioNTech COVID-19 vaccine.
The compositions of the lipid nanoparticles are very similar for the two vaccines (Pfizer/BioNTech and Moderna): an ionizable cationic lipid, a PEGylated lipid, cholesterol, and the phospholipid distearoylphosphatidylcholine (DSPC) as a helper lipid.”
https://www.cas.org/resource/blog/understanding-nanotechnology-covid-19-vaccines
From a Frontiers article reviewing the development and delivery systems for mRNA vaccines, they present a brief summary of a 2018 study funded by both Moderna and AstraZeneca. The study was looking into the safety of the liposome nanoparticles used to carry the mRNA in the vaccines. It found evidence of pro-inflammatory responses in both monkeys and rats:
Development and Delivery Systems of mRNA Vaccines
“Maja et al. (2018) evaluated the safety of LNP packaging of human erythropoietin (hEPO) mRNA in monkeys and rats. following intravenous injection of 0.3 mg/kg mRNA LNP, hEPO levels were highest at 6 h post-infusion and exceeded the expected effective exposure 100-fold at the maximal dose. Active hEPO protein was detected in both rats and monkeys, indicated by significant increase in erythrocyte mass. Some increase in white blood cell count, changes in coagulation parameters, liver injury and release of IFN-γ-induced protein were observed in rats, while in monkeys, splenic necrosis, lymphocyte depletion and mild, reversible complement activation were observed. These pro-inflammatory responses may be minimized by reducing the dose or the frequency of administration.”
https://www.frontiersin.org/articles/10.3389/fbioe.2021.718753/full
Polyethylene Glycol (PEG)
PEG is used as a coating and as a stabilizer to the lipid nanoparticles. It is found in numerous products ranging from cosmetics to food. However, it is a known toxin and has led to anaphylaxis in many people allergic to it:
Anaphylaxis to Pfizer/BioNTech mRNA COVID-19 Vaccine in a Patient With Clinically Confirmed PEG Allergy
“Polyethylene glycol (PEG) is a hydrophilic polymer incorporated in the form of lipid-PEG conjugates in both of the mRNA COVID-19 vaccines from Pfizer/BioNTech and Moderna to stabilize the lipid nanoparticles carrying the mRNA (1–3). PEG is routinely used in the formulation of protein drugs and nanomedicines to reduce aggregation and improve distribution and elimination kinetics (4–8). Allergic reactions to PEG have been noted for several PEGylated drugs, leading to adverse events ranging from infusion reactions to anaphylaxis (9–13). There have also been numerous reports of allergic responses to PEGs present in a diverse group of goods, ranging from osmotic laxatives to soaps, lotions, and cosmetics, as well as to other pharmaceuticals such as analgesics, depo injections, laxatives, and various tablet formulations of drugs such as antacids and antibiotics, which may include PEG as an excipient (14–17).
Since allergic reactions to vaccines are exceptionally rare [~1.3 cases per million doses (18)], when several cases of anaphylaxis to the Pfizer/BioNTech and Moderna vaccines were noted soon after rollout, there were speculations that the response might be attributed to PEG sensitivity (19–21). The link between anaphylaxis to the vaccines and PEG-hypersensitivity was recently reported for one individual in the U.K. (22). Here, we report another case of an individual with a PEG-allergy that was identified after experiencing anaphylaxis to the Pfizer/BioNTech COVID-19 vaccine.”
“This report describes anaphylaxis to the Pfizer/BioNTech COVID-19 vaccine in a patient who was later confirmed to be allergic to polyethylene glycol. This report adds to several other recent publications describing PEG allergy-related reactions to mRNA COVID-19 vaccines (22, 24, 25), supporting the need for individuals with suspected allergy to PEG to consult an allergist prior to vaccination. Individuals with a history of anaphylactoid reactions to several different types of drugs should raise suspicion for allergy to excipients that may be common across formulations, such as PEG.”
https://www.frontiersin.org/articles/10.3389/falgy.2021.715844/full
Acetic Acid
Acetic acid is the chemical component in vinegar which causes it to burn upon contact with the skin. It is used as a pH stabilizer in the vaccines. It would seem obvious not to inject the acid that makes vinegar burn directly into the body, however here we are injecting this corrosive poison directly into the body:
Glacial Acetic Acid Adverse Events: Case Reports and Review of the Literature
“Glacial acetic acid is a dangerous chemical that has been associated with several adverse drug events involving patients over recent years. When diluted to the proper concentration, acetic acid solutions have a variety of medicinal uses. Unfortunately, despite warnings, the improper dilution of concentrated glacial acetic acid has resulted in severe burns and other related morbidities.”
“Although classified as a weak acid, glacial acetic acid is a corrosive poison that can cause injury or death when human tissue is exposed to it. At concentrations of 10% to 25% (1.67-4.16 mol/L), it acts as an irritant; but at concentrations greater than 25% (>4.16 mol/L), it is corrosive and should be handled in a fume hood.2 Skin contact may produce blistering or burns, while liquid or spray mist may produce tissue damage particularly on mucous membranes of the eyes, mouth, and respiratory tract. 3“
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4589881/#__ffn_sectitle
The Experimental Findings of mRNA Vaccines

Finally, in April 2019, a study came out comparing plasmid DNA and mRNA vaccines. It is a very comprehensive review and details many of the challenges in creating a vaccine as well as the unknowns and potential toxicities involved. It details the greater inflammatory response associated with the mRNA technology as well as the instability of the mRNA which has led researchers away from its use in the past. The inflammatory effects are considered potential detrimental effects and the use of repeated doses is questioned due to supposedly quick degradation of mRNA in the body. It also provides some breakdowns of key finding from several studies relating to the dangers involved with its use.:
A Comparison of Plasmid DNA and mRNA as Vaccine Technologies
Abstract
“This review provides a comparison of the theoretical issues and experimental findings for plasmid DNA and mRNA vaccine technologies. While both have been under development since the 1990s, in recent years, significant excitement has turned to mRNA despite the licensure of several veterinary DNA vaccines. Both have required efforts to increase their potency either via manipulating the plasmid DNA and the mRNA directly or through the addition of adjuvants or immunomodulators as well as delivery systems and formulations. The greater inherent inflammatory nature of the mRNA vaccines is discussed for both its potential immunological utility for vaccines and for the potential toxicity.”
“This instability of mRNA has been a significant reason for the lack of interest in mRNA as a drug. In addition, RNA has long been known to be an immunologically active molecule. For example, poly (I:C) (polyinosine-polycytidylic acid) is a synthetic analog of dsRNA (double-stranded RNA) that is an agonist of TLR3 and has long been used as an immunostimulatory mimic of viral infection and tested as an adjuvant to increase immune responses for experimental vaccines [13,14,15]. mRNA has a number of immunostimulatory mechanisms, which may be useful—or detrimental—for mRNA used for vaccines or cancer immunotherapeutics (discussed below).”
6. Cellular Targets for mRNA and Plasmid DNA Vaccine Delivery
“For many vaccines, antibodies play a key role in protection. The cell that is transfected by the plasmid DNA or the mRNA vaccine does not have to be a professional antigen presenting cell (APC) in order to produce the antigenic protein that stimulates B cells. Cellular immune responses, notably CTLs, are thought to be important for tumor immunotherapy as well as to potentially play a role in protection against certain infectious diseases, e.g., tuberculosis (Tb), HIV, and malaria, or for vaccines effective against multiple strains of a virus, such as influenza, even though CTLs alone would not provide sterilizing immunity.
Plasmid DNA was shown to be effective for stimulating CTLs that were capable of protecting mice against influenza caused by a strain different from the strain from which the encoded antigen was derived [7,27,28]. Because the plasmid DNA, when injected intramuscularly (i.m.), primarily transduced muscle cells rather than professional Antigen Presenting Cells (APCs), the mechanism whereby MHC Class I-restricted CTLs were generated needed explaining. It was found that cross-priming appeared to be a key mechanism for generating CTLs following DNA vaccine immunization, as directly demonstrated by experiments with chimeric mice using bone-marrow derived dendritic cells [27], and because muscle cells were the only cells observed to translate the protein encoded by directly-injected plasmid DNA [6,29]. The efficacy in pre-clinical models raised the hopes that such plasmid DNA-based CTL-inducing vaccines could be developed that would be protective against multiple strains of HIV or influenza [7,30] (so as to produce a “universal” flu vaccine). Currently, existing influenza vaccines depend upon strain-specific antibodies, which result in strain-specific or strain-limited protection. Similarly, mRNA delivered in liposomes was shown early on to be capable of inducing CTLs [9]. The uptake of the mRNA is also mainly by non-immune cells, including muscle cells [31].“
8. Inflammatory Responses and Toxicities
8.1. Immune Activation
“As noted above, the use of modified nucleosides for the construction of mRNA is one method of decreasing the reactogenicity of the in vitro transcribed mRNA. However, mRNA acts via multiple pathways, including the innate system (via TLR3, TLR 7, and TLR8) and via cytoplasmic proteins (PKR, OAS, RIG-I, and MDA5) [11,51]. The multiple routes of activation result in several effects in addition to inflammation and include inhibition of mRNA replication (both via TLR7 through an MYD88 pathway affecting interferon, and via TLR3 through TRIF), stalled translation, and RNA degradation [5]. Some of these various activities could decrease the potency of the mRNA by a net decreased protein production, as was seen pre-clinically for an HIV mRNA vaccine complexed in cationic lipids [52]. This also raises the issue of how effective repeat dosing of mRNA will be if previous injections result in an environment with decreased translation or increased RNA degradation, although simply changing an injection site may potentially circumvent this particular issue.
Other molecular entities that are introduced or generated during the manufacture of the in vitro-transcribed mRNA and then remain (left-over contaminating nucleoside triphosphates, DNA templates, and dsRNA) are also quite immunostimulatory and therefore need to be purified following production of the mRNA [53].
The potential issues due to the various inflammatory effects of mRNA vaccines upon clinical efficacy and safety are summarized in Table 2 and are discussed below.”

8.2. Toxicities of mRNA
The flip side of the possibly beneficial adjuvant inflammation, however, is potential toxicity of the mRNA vaccines. Toxicities are seen with antivirals and anti-cancer drugs that contain unnatural nucleoside analogues [56,57,58]. Such toxicities, not predicted by pre-clinical studies due to species differences between humans and the animals used for pre-clinical safety testing, have been seen with drugs that contain unnatural modified nucleosides. The clinical adverse effects have included myopathy (caused by mitochondrial toxicity), lactic acidosis, pancreatitis, lipodystrophy, liver steatosis, and nerve damage; certain ones have been fatal.
Indeed, some toxicity has been reported for mRNA pre-clinically along with limited human adverse events. Liver toxicity was observed in pre-clinical studies with one potential mRNA therapeutic delivered in lipid nanoparticles for Crigler-Najjar syndrome, selected as a “lowest-hanging fruit” target because very low doses of protein were needed. These were serious enough to apparently halt the work with this particular entity, or at least that formulation [59]. The formulation of the mRNA was thought to potentially play a role in the toxicity [60], and repeat doses were used. Nevertheless, this observed toxicity may be concerning for vaccines as well, since even live replicating viruses and viral vector vaccines (which generally are more immunogenic than subunit vaccines) need repeat dosing. In addition, most of the mRNA vaccines in clinical trials appear to need formulation. The mRNA vaccines in clinical trials against infectious diseases from this same company are described as formulated in lipid nanoparticles, but whether they are the same formulations as those used for the Crigler-Najjar study is not publicly known.
Self-limited local and systemic adverse events (AEs) seen in a human clinical trial for an mRNA rabies vaccine, although summarized as still indicating the vaccine was generally safe (described below in the clinical trials section), may also reflect the inflammatory nature of the mRNA [55]. These results highlight the potential toxicity downside of the inflammatory activity of mRNA vaccines, adverse effects not seen to this extent with plasmid DNA. Also note that, for providing monoclonal antibodies [61] (whether for preventing or for treating infectious diseases for other therapeutic applications), this would likely require repeat administration of mRNA, which might not only increase the potential for toxicities, but may also have an impact upon potency due to effects of the mRNA upon decreasing translation, etc., via the other inflammatory effects.
Thus, it may still be a work in progress to find the best balance of inflammation and any deleterious toxicities via harnessing adjuvant activities of mRNA while limiting or suppressing inherent toxicities for vaccines and immunotherapeutics. This will involve optimizing nucleoside substitutions, the design of other elements of the mRNA construct, any included immunostimulants, and/or specific formulations, delivery devices, and routes of administration. The mechanisms of mRNA inflammation that are relevant to their potential efficacy and safety as vaccines are also reviewed elsewhere [34], where they are aptly referred to as the “yin and yang of innate immunity.”
“For mRNA, a proposed mechanism for possible autoimmune responses is via the induction of type I interferon [63], which may result in both inflammation and possibly autoimmune responses [64]. This includes work showing that the responses seen in mice were similar to those seen in humans for an influenza mRNA vaccine construct via TLR7 and TLR8 in humans and via cytoplasmic RNA sensors in both mice and humans [65].”
10.2. RNA
10.2.1. Prophylactic mRNA Vaccines for Infectious Diseases
“Prophylactic vaccine human trials for infectious diseases utilizing mRNA encoding the antigen(s) are shown in Table 3. These are all Phase I trials. Any known formulations are listed, as are any described results and references, along with the clinical trials identifier numbers. The rabies vaccine effort utilizing a licensed vaccine with RNA as the adjuvant (discussed above, and listed in Table 4) was replaced by a vaccine using mRNA encoding the rabies virus glycoprotein. Following either i.d. or i.m. injection of this rabies mRNA vaccine, boostable antibodies were obtained. However, 78% of each group had “solicited systemic adverse events” including ten patients (~10% of all injected patients) with grade three (i.e., serious but not life-threatening) adverse events, although the conclusion was that the vaccine was “generally safe with a reasonable tolerability profile” [55]. A second construct for rabies is now in clinical testing.”
11. Summary and Conclusions
“In summary, despite all the excitement over pre-clinical efficacy of mRNA, it should be remembered that in many ways, the mRNA field is recapitulating what occurred with plasmid DNA 20+ years ago, when seemingly almost any disease could be prevented or treated in pre-clinical animal disease models with the administration of an unformulated plasmid encoding a key antigen [1]. Therefore, one must keep in mind that pre-clinical immunogenicity or even protection/therapy, and human immunogenicity are low hurdles and are not predictive of human efficacy. One reason this is so challenging is that, for many of the diseases under evaluation, scientists do not know which immune response or combination of immune responses and which antigen targets are the crucial elements for efficacy; the vaccine technology alone is not the only piece of the puzzle. Table 5 summarizes the main advantages and disadvantages of mRNA vaccines with a comparison to DNA vaccines.”

“One should also not ignore the reported toxicities seen with the rabies mRNA vaccine [55] that included limited systemic AEs for the majority of patients (78%) and even grade three AEs in ~10% of patients following doses of 80–400 μg mRNA via different routes, although the conclusions were that the vaccine was generally safe. It is not known whether the pre-clinical hepatic toxicity that proved to be a “no go” result for a particular Crigler-Najjar mRNA candidate is relevant to the mRNA vaccine studies from the same company, because, despite the low doses used, the doses and mRNA formulation for vaccine studies may be different. This is in comparison to DNA vaccine clinical trials where 4 mg doses of DNA i.m. with boosts have been used in a variety of clinical trials with limited systemic symptoms [83,84,85] while generating good immune responses.
Just as DNA vaccines, after more than 25 years since the first publication of preclinical protective efficacy, are still a work in progress in improving potency and finding the right antigens and targets, there remain challenges for mRNA to become clinical products. For both DNA and mRNA vaccines (and monoclonal antibodies and bi-specific antibodies before them), a simple concept may have a challenging path to reality, and the technology may not be totally generic. mRNA may be even more complex than plasmid DNA because of the modifications (modified nucleosides) plus the formulations needed for stability, delivery, and the need to control the innate immunostimulatory activity of the mRNA. However, it also offers advantages in terms of manufacture that avoids the need for any animal or cellular products. The hope is that once the fundamental key challenges are solved for both plasmid DNA and mRNA, the clinical successes will come rapidly, although that has not occurred for moving from the veterinary licensed products for DNA vaccines into humans, demonstrating how much still needs to be understood, not just about the technologies but about the diseases that are being treated or prevented.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6631684/
In Summary:
- According to mRNA inventor Robert Malone, the CDC and the FDA are “profoundly corrupt” and are forcefully pushing experimental gene therapeutics, aka “COVID” vaccines, on the population with “grossly incomplete” data that does not meet even the “minimum standards” for safety
- According to Moderna, they developed proprietary technologies and methods to create mRNA sequences that cells recognize as if they were produced in the body
- This is how Moderna describes how they create their vaccines:
- They start with the desired sequence for a protein.
- They design and synthesize the corresponding mRNA sequence.
- They engineer that mRNA sequence to optimize the mRNA’s physical properties, as well as those of the encoded protein.
- They deliver the mRNA sequence to the cells responsible for making that protein via one of several modalities (in this case, lipid nanoparticles).
- Once the mRNA – the instructions – are in the cell … human biology takes over, ribosomes read the code and build the protein, and the cells express the protein in the body (that’s the theory behind what happens as they can not observe this)
- According to the CDC, mRNA vaccines use mRNA created in a laboratory to teach our cells how to make a protein—or even just a piece of a protein—that triggers an immune response inside our bodies:
- The mRNA will enter the muscle cells and instruct the cells’ machinery to produce a “harmless” piece of what is called the spike protein
- Our immune system recognizes that the protein doesn’t belong there which triggers our immune system to produce antibodies and activate other immune cells to fight off what it thinks is an infection
- At the end of the process, our bodies have learned how to protect against future infection from the virus that causes COVID-19
- Of course, we get the obligatory “any temporary discomfort experienced after getting the vaccine is a natural part of the process and an indication that the vaccine is working” warning (a.k.a. lie)
- According to the AAMC, the theory behind the vaccines is that mRNA will tell a cell to make a protein that’s used by a certain “virus,” which would set off an immune response that builds the body’s ability to fend off the actual “virus”
- The theory showed promise in lab experiments and animal trials through the 1990s and early 2000s
- Several stubborn drawbacks impeded the technology’s usefulness:
- It was difficult to get mRNA into a cell
- mRNA caused severe inflammation and was quickly degraded by the body
- To overcome these hurdles, they used synthetic RNA that the body’s immune system doesn’t recognize and encased that material in lipid nanoparticles (fat bubbles) that easily slip into cells
- According to Moderna in 2018, in theory, mRNA could prompt proteins to be made in the body and would put the drug factory inside of a person
- Moderna’s slick storytelling helped to raise over $1.7 billion—all from private investors
- It has also invited skeptics, who would like to see those ambitions backed up by data
- Moderna thought they had overcome some of the fundamental challenges of translating mRNA from idea to product
- Various ingredients in the vaccines are known toxins
- Lipid nanoparticles have an unwanted side-effect; they have the potential to induce an allergic reaction, particularly for those who suffer with severe allergies.
- A 2018 study (funded by Moderna and AstraZeneca) examining the safety of the Liposome Nanoparticle mRNA delivery system found:
- Some increase in white blood cell count
- Changes in coagulation parameters
- Liver injury and release of IFN-γ-induced protein were observed in rats
- Splenic necrosis, lymphocyte depletion and mild, reversible complement activation were observed in monkeys
- These pro-inflammatory responses may be minimized by reducing the dose or the frequency of administration
- Polyethylene glycol (PEG) is a hydrophilic polymer incorporated in the form of lipid-PEG conjugates in both of the mRNA COVID-19 vaccines from Pfizer/BioNTech and Moderna to stabilize the lipid nanoparticles carrying the mRNA
- Allergic reactions to PEG have been noted for several PEGylated drugs, leading to adverse events ranging from infusion reactions to anaphylaxis
- There have also been numerous reports of allergic responses to PEGs present in a diverse group of goods, ranging from osmotic laxatives to soaps, lotions, and cosmetics, as well as to other pharmaceuticals
- When several cases of anaphylaxis to the Pfizer/BioNTech and Moderna vaccines were noted soon after rollout, there were speculations that the response might be attributed to PEG sensitivity
- The report described anaphylaxis to the Pfizer/BioNTech COVID-19 vaccine in a patient who was later confirmed to be allergic to polyethylene glycol which added to several other recent publications describing PEG allergy-related reactions to mRNA “COVID-19” vaccines
- Glacial acetic acid is a dangerous chemical that has been associated with several adverse drug events involving patients over recent years
- The improper dilution of concentrated glacial acetic acid has resulted in severe burns and other related morbidities
- Although classified as a weak acid, glacial acetic acid is a corrosive poison that can cause injury or death when human tissue is exposed to it
- Skin contact may produce blistering or burns, while liquid or spray mist may produce tissue damage particularly on mucous membranes of the eyes, mouth, and respiratory tract
- An April 2019 study provided a comparison of the theoretical issues and experimental findings for plasmid DNA and mRNA vaccine technologies
- The greater inherent inflammatory nature of the mRNA vaccines was discussed for both its potential immunological utility for vaccines and for the potential toxicity
- The instability of mRNA has been a significant reason for the lack of interest in mRNA as a drug
- In addition, RNA has long been known to be an immunologically active molecule
- Cellular immune responses, notably CTLs, are thought to be important for tumor immunotherapy as well as to potentially play a role in protection against certain infectious diseases, e.g., tuberculosis (Tb), HIV, and malaria, or for vaccines effective against multiple strains of a “virus,” such as influenza, even though CTLs alone would not provide sterilizing immunity
- Plasmid DNA, when injected intramuscularly (i.m.), primarily transduced muscle cells rather than professional Antigen Presenting Cells (APCs)
- Similarly, mRNA delivered in liposomes was shown early on to be capable of inducing CTLs and the uptake of the mRNA is also mainly by non-immune cells, including muscle cells
- The multiple routes of mRNA activation result in several effects in addition to inflammation and include inhibition of mRNA replication, stalled translation, and RNA degradation
- This raises the issue of how effective repeat dosing of mRNA will be if previous injections result in an environment with decreased translation or increased RNA degradation
- Other molecular entities that are introduced or generated during the manufacture of the in vitro-transcribed mRNA and then remain (left-over contaminating nucleoside triphosphates, DNA templates, and dsRNA) are also quite immunostimulatory
- There are potential issues due to the various inflammatory effects of mRNA vaccines upon clinical efficacy and safety
- The flip side of the “possibly beneficial adjuvant inflammation,” is potential toxicity of the mRNA vaccines
- The clinical adverse effects of unnatural nucleoside analogues have included:
- Myopathy (caused by mitochondrial toxicity)
- Lactic acidosis
- Pancreatitis
- Lipodystrophy
- Liver steatosis
- Nerve damage
- Death
- Liver toxicity was observed in pre-clinical studies with one potential mRNA therapeutic delivered in lipid nanoparticles for Crigler-Najjar syndrome which were serious enough to apparently halt the work with this particular entity, or at least that formulation
- The formulation of the mRNA was thought to potentially play a role in the toxicity and repeat doses were used
- Self-limited local and systemic adverse events (AEs) seen in a human clinical trial for an mRNA rabies vaccine, may also reflect the inflammatory nature of the mRNA
- These results highlight the potential toxicity downside of the inflammatory activity of mRNA vaccines
- This would likely require repeat administration of mRNA, which might not only increase the potential for toxicities, but may also have an impact upon potency due to effects of the mRNA upon decreasing translation, etc., via the other inflammatory effects
- It is still be a work in progress to find the best balance of inflammation and any deleterious toxicities via harnessing adjuvant activities of mRNA while limiting or suppressing inherent toxicities for vaccines and immunotherapeutics
- For mRNA, a proposed mechanism for possible autoimmune responses is via the induction of type I interferon, which may result in both inflammation and possibly autoimmune responses
- In a rabies mRNA vaccine trial, 78% of each group had “solicited systemic adverse events” including ten patients (~10% of all injected patients) with grade three (i.e., serious but not life-threatening) adverse events
- It must keep in mind that pre-clinical immunogenicity or even protection/therapy, and human immunogenicity are low hurdles and are not predictive of human efficacy
- One reason this is so challenging is that, for many of the diseases under evaluation, scientists do not know which immune response or combination of immune responses and which antigen targets are the crucial elements for efficacy
- One should also not ignore the reported toxicities seen with the rabies mRNA vaccine
- It is not known whether the pre-clinical hepatic toxicity that proved to be a “no go” result for a particular Crigler-Najjar mRNA candidate is relevant to the mRNA vaccine studies from the same company
- There remain challenges for mRNA to become clinical products
- mRNA may be even more complex than plasmid DNA because of the modifications (modified nucleosides) plus the formulations needed for stability, delivery, and the need to control the innate immunostimulatory activity of the mRNA
- The challenges related to DNA and mRNA vaccines demonstrates how much still needs to be understood, not just about the technologies but about the diseases that are being treated or prevented
It seems pretty obvious when doing a quick breakdown of the mRNA technology why the inventor of this process has so many concerns regarding its use. This is experimental technology that is based upon theoretical guesses as to what these injections will do once inside a human body. Previous experiments have shown toxic effects on animals and humans involved in different trials. Various ingredients used in its creation are known toxins with proven severe reactions. The synthetic lab-created mRNA are known to produce strong inflammatory responses which are assumed to be signs of success but are in fact the normal response of a body poisoned by foreign substances. Numerous instances of severe, life-threatening, and fatal reactions are being reported in far greater quantities than for any vaccine that has come before. Warning labels have already been added for anaphylaxis, blood clots, and myocarditis. Guillain-barre syndrome has become associated with the use of these gene-therapies masquerading as vaccines.
The known dangers coupled with the unknowns should be enough to at least question its use. Taken together with the fact that “SARS-COV-2” was never properly purified/isolated nor proven pathogenic and exists only as random A,C,T,G’s in a computer database, every single person waiting in line for these lab-created cocktails should immediately forget about the free donuts, gas, money, candy or whatever other ridiculous incentives they throw out there to coax one into a life-altering decision, and simply turn around and walk away.


Outrageous that world Governments are mandating these poisons. They are making life impossible for people who are not vaccinated.
LikeLiked by 1 person
It is absolutely outrageous that people are being coerced and feeling forced into a medical decision that can significantly impact their lives in order to work, to travel, to enjoy entertainment, etc. No one should feel compelled to do something they deem is not in their best interest. I’m alarmed more people are not up in arms over this and have accepted it. It’s frustrating.
LikeLike
If this MRNA gene therapy was so great, why would you need immunity for liability? Answer cause its a killer !and they know it !
LikeLiked by 1 person
Absolutely. They would not need complete protection if they knew it was safe and effective. Why people continue to trust these criminals is beyond me.
LikeLike
What an IDIOT God (the all-knowing source of reality) was when he created humans! We need to fix God’s sloppy, poorly done job, with manmade chemicals and solutions!
But I guess they (the mainstream sources) also want God to play an absolutely minimal role in one’s worldview, partially because serving only one God, as opposed to the government and “infallible” (but also constantly changing and backtracking) Science (proper noun) is a threat to them.
LikeLiked by 1 person
Exactly. Everything they do is attempting to lead people away from God.
LikeLike