If you’ve been paying close attention to the evidence used to sell the public on this “pandemic” over the last few years, it should have been obvious from the start that there was never a new “virus” spreading across the world leaving death and destruction in its wake. You would have seen from the original studies that the suspected novel “virus” was never purified and isolated directly from the fluids of a single sick patient nor was it ever proven pathogenic. You would have determined that the genome of the “virus” was nothing more than the Frankensteined amalgamation of RNA from numerous sources cobbled together by consensus sequencing, alignment, and computer algorithms. You would have discovered that the PCR tests were based directly on this fabricated genome and that they were never once calibrated and validated against the gold standard of purified and isolated “virus” particles. Because of this, the test can only produce false-positive results and erroneous cases. Thus, if you are an intellectually honest person, there could only have been one logical conclusion to make. This is and has always been a Testing Pandemic and was never a “viral” one.
If you did find yourself at this logical conclusion and you felt compelled to share this information with your loved ones, you are all too aware of the typical responses which followed:

Those of us who have tried to get this information out to friends, family, and the public at large have been ridiculed, harassed, and in some cases threatened. We have been labelled as conspiracy theorists and have suffered broken relationships. Some have had to give up careers in order to get the truth out into a world that has largely shunned those of us speaking out and has fought back against the message we have presented. We have witnessed a strong cognitive dissonance in those who are unwilling to challenge the Germ Theory narrative that has been indoctrinated into us from birth. People cling to this delusion and defend it with a ferocious anger. They are either not ready or are unwilling to discover for themselves whether the information presented by the pharmaceutically-controlled mainstream media and public health officials is in fact trustworthy. They would rather “trust the science” than discern the truth for themselves through critical thought and logic.

For anyone who has been reluctant to listen to those of us who have tried to reach out because we do not fit some preconceived notion of authority and/or expertise, a recently released study submitted to the highly regarded scientific journal The Lancet may fit the bill. As it was founded in 1823, The Lancet is one of the oldest weekly peer-reviewed medical journals and it is also among the most respected as well. It would not benefit their long-standing prestigious reputation to publish a study promoting “conspiracy theories.” However, it appears that they may have just done that in November 2021.
The study presented below checks nearly every box off of the “conspiracy theory” checklist.
- Lack of a purified/isolated “SARS-COV-2.” ✔️
- Genome created from mixed RNA sources. ✔️
- PCR tests based off of the fraudulent genome and never calibrated against purified/isolated “viruses.” ✔️
- All PCR positives are false-positives. ✔️
- Masks have been proven ineffective based on 100+ years of knowledge. ✔️
- Vaccination is ineffecttive and harmful. ✔️
Sadly, the researchers do attempt to hypothesize that it is in fact due to exosomes that the tests are inaccurate and that the vaccines are ineffective. Exosomes are said to be extracellular vesicles that are secreted by cells and act as a communication system within the body. They are the exact same size, shape, and morphology as “viruses” and are considered to be essentially non-infectious “viruses.” The problem with this theory, however, is that one can not use fictional entities (exosomes) to prove and/or invalidate other fictional entities (“viruses”). Just like their identical counterparts, exosomes have never been properly purified and isolated and their functions are entirely theoretical. Even with the belief that exosome RNA is responsible for the “SARS-COV-2” genome and the admitted lack of proof of any purified/isolated “SARS-COV-2,” the researchers still acknowledge the supposed existence of the “virus” as well as the disease known as “Covid-19.” Still, whether you agree with the hypothesis or not, it is an interesting paper that dismantles many of the mainstream narratives surrounding this hoax. The entire paper is presented below followed by a summary:
Role of exosomes in false-positive covid-19 PCR tests: non-specificity of SARS-CoV-2-RNA in vivo detection explains artificial post-pandemic peaks
Summary
Background: The COVID-19 pandemic priorities have focused on prevention by detection and response. National governments’ prevention response decisions are based upon detection statistics from PCR tests that are used to define numbers of (i) COVID-19 infected persons, (ii) COVID-19 hospitalisations, and (iii) COVID-19 deaths. These statistics assume a priori that PCR tests are nigh 100% true detectors of COVID-19 infections. Here we will provide an alternative interpretation, along with the compelling evidence, that false positives have distorted to some degree the statistics of the primary outbreaks, and account for almost the whole of the 2nd and subsequent apparent COVID-19 outbreak peaks in various countries.
Methods: We extract from the published literature on PCR-test outcomes graphical data that reveals the evidence for a very large percentage of false positive results. We review the role of exosomes in the immune response to all respiratory viral infections and its effect on PCR tests. We hypothesise that exosomes, triggered by all viral respiratory infections, are largely responsible for positive outcomes from PCR-tests for COVID-19. We test our alternative interpretation for consistency with the
empirical epidemiological trends as published by WHO.
Findings: We find that PCR testing data for the second and following waves of COVID-19 pandemic indicate that these waves are mainly artefacts of false-positive results. We find that this interpretation provides a more consistent explanation of the known epidemiology of COVID-19 than the hitherto consensus notion of extremely contagious and quickly mutating viruses.
Interpretation: The RNA code counted in PCR tests, previously attributed to SARS-CoV-2, belongs instead to a respiratory-virus-induced immune system response by human cells that liberate exosomes, and that vitiate PCR test results. PCR tests have
zero specificity in vivo due to the exosome RNA. PCR tests exhibit excellent specificity in vitro on pure samples of other respiratory viruses. Low success rate of vaccines is explained by inexact identification of the SARS-CoV-2 RNA.
INTRODUCTION
Recently the World Health Organisation (WHO) published a document that called attention to the relevance of false positive results of Reverse transcription (RT-) Polymerase Chain Reaction, (PCR) tests for a SARS-CoV-2 virus, the causing agent of respiratory disease commonly known as COVID-19. PCR tests are used to directly screen for the presence of viral RNA, which will be detectable in the body before antibodies form or symptoms of the disease are present. During PCR testing for COVID-19, substances known as reverse transcriptase or DNA polymerase are added to a nasopharyngeal sample in a lab. These substances work to make numerous copies of any viral RNA that may be present. This procedure ensures enough copies of the RNA are present to signal a positive result, as specifically designed primers and
probes attach themselves to sequences of the genetic code of the virus to signal that a pathogen has been found.
The WHO publication is a reminder that the disease prevalence alters the predictive value of test results. As disease prevalence decreases, the risk of false positive increases. This means (quote) “that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity” (underlined by us). The WHO alarm notification has been vindicated by a field-study investigation in UK.
In layman terms, technical specifications provided by test producers becomes irrelevant at low SARS-CoV-2 prevalence. The producers may claim their test is 100% specific to the SARS-CoV-2 virus, but in practice if COVID-19 prevalence in the population is low or zero – as may well happen seasonally – each and every positive result will be a false positive, reducing the amount of information contained in it to zero. Note, however, that since the start of the pandemic, the WHO has been proclaiming that more extensive testing is necessary, which could conceivably generate ever repeating unreal ‘COVID-19 outbreaks’.
The warning signals already have important consequences for public health institutions, which could have far-reaching damaging effects not just to public health services but to the general economy of political decisions based upon PCR test statistics. We note the following 4-point established facts at the outset.
- Irrespective of the test specificity claimed by the test manufacturer, PCR tests produce false positive results in appreciable numbers.
- The fraction of false positive results in all positive results increases as the prevalence of the SARS-CoV-2 virus in the population decreases, e.g. due to seasonality of all other respiratory infections;
- In the limiting case of zero prevalence of SARS-CoV-2 virus, all positive PCR test results will inevitably be false positives;
- PCR tests can never indicate that SARS-CoV-2 virus went out of circulation, as false positives will be appearing indefinitely, indicating alleged presence of the virus.
Accordingly, we have investigated a more plausible explanation for the
development of COVID-19 pandemic data since 2019, based upon the alternative interpretation that exosomes play a role in false positive tests of patients that do not carry the COVID-19 virus. We find that the prevailing interpretation of PCR test results does not withstand scientific scrutiny in the light of the experimental or factual observations.

EXOSOMES
The important role of exosomes in the functioning of the immune system challenged by a viral respiratory disease is established science, although the precise function and molecular mechanisms remain a topical research question. Cells challenged by viruses produce exosomes, apparently signaling the immune system into action. Exosomes are structurally like a flu virus and contain some information in form of RNA and some attached proteins that provide structural integrity and acceptance by the target cells of the immune system. The immune response to respiratory viruses is evidently triggered by the appearance of exosomes.
The trigger may also involve individual airway epithelial cells, at least partly, as exosomes were found to contain viral proteins, although only not the beginning of the illness, indicating that interaction with the immune is necessary before that happens. Generally, foreign viral RNA may be identified by comparing it to cell’s own genetic material. Such function requires specialized cellular machinery, hardly compatible with normal physiological function of epithelial cells.
Exosomes, however, contain the answer to the ‘where’ question, and
information contained in the exosome RNA should uniquely identify the virus-challenged airway epithelial cells, allowing the immune system to prepare its targeted response. The exosome RNA structure is probably independent of the pathogenic virus and varies only in conformity with the patients’ individual genome.
These patient genome variations consistently explain several observations, which the consensus hypothesis attributes to the special properties of SARS-COV-2. Indeed, any test would produce negative outcome for exosomes whose RNA is different from that of the exosomes used for developing the test. This explains the 40% false negatives reported in China at the outset of the pandemics, in patients with classical clinical symptoms of COVID-19.
On the other hand, sequencing of the perceived viral RNA in remote locations necessarily reveals new exosome strains, caused by human genetic variability, but misidentified as new SARS-COV-2 variants. Once tests detecting such exosomes are developed and deployed, these perceived virus variants get instantly discovered everywhere, creating a false and terrifying impression of their fast propagation. The apparent propagation rate of such new variants will only be limited by the throughput of the testing system. Many differing human genomes coexist in various geographic locations due to modern population mobility.
These variant-specific tests would also produce false negatives on patients with differing genomes, albeit on genomes different from the undetectable genomes of the original tests. The exosome origin of the RNA attributed to SARS-COV-2 and its variants explains the fact that PCR tests used on patient biological samples are completely non-specific as regards the virus. Indeed, these tests are specific to exosome RNA, which probably carries no virus information, as postulated above. This, in turn, explains a misdiagnosis phenomenon, that manifests itself in countless observations the more salient of which we itemise and outline in the following section.
OBSERVATIONS EXPLAINED
We describe as ‘false positive multiplication by compulsory contact testing'(FPMCCT) and requires no further explanation. The second is one of the key points of the present paper and is described as illnesses caused by seasonal respiratory viruses, including variants of influenza A and B, common cold rhinoviruses, human corona viruses, etc. all being ‘misdiagnosed by PCR tests as SARS-CoV-2 virus’ (MDSCV), with very high probabilities, close to 100%. This phenomenon will be discussed below in more detail.
The following published records of information were obtained from
mainstream media and, verified with Our World in Data, wherever quantitative data was called for. The order in which the salient questions asked is arbitrary.





We can apply the scientific method criteria to analyse the pandemic data, with WHO observations/questions, and alternative OPS explanations, itemised in the previous section, objectively. From the point of view of the scientific method defined above
we note that is has not been adhered by scientific advisors to many national governments that have already answered “yes” to the many questions raised by the WHO in ad hoc knee-jerk responses to the pandemic.
The interpretations provided by OPS explanations are compliant with the scientific-method criteria. Unlike WHO, we are not using any alleged or unsubstantiated properties, e.g., hypothetical rate-of-transmission of SARS-CoV-2 variants. We refer only to information demonstrably correct, however, we question the reliability of analytical tools existing at the present time, like dubious PCR tests. However, the proposed role of exosomes in the false-positive PCR test results will
remain a hypothesis that needs to be investigated with some circumspection for more direct laboratory experimental evidence that it is the agent responsible for vitiating PCR test results.
The WHO interpretations require the following hypothetical assumptions for which there is presently no compelling evidence: going against the principle of Occam’s razor:
- Transmission by asymptomatic COVID-19 carriers
- Tests working and being 100% specific in clinical in vivo practice
- Vaccines are effective: vaccinated people are getting ‘infected’.
- Effectiveness of vaccines defined by PCR test?
- The same virus generating completely different outbreak dynamics in the first and subsequent waves. The OPS explanations only assume established scientific knowledge that has been conclusively demonstrated:
- PCR Tests produce false positives both on different respiratory viruses and on patients having no respiratory viruses at all
- Contact PCR testing amplifies number of tests and of false positives
- Classic, or nearly Gaussian, dynamics of the first (SARS-CoV-2) wave in 2020 (March-May in Western Europe), and the slower-skewed testing–generated dynamics in the subsequent waves
The observations, and consensus interpretations that we question above, are somewhat contradictory. Compare, for example, items 5, 7 and 10, in which the assumptions that public health measures were both sufficient and insufficient, to reduce propagation of SARS-CoV-2 are questioned. Also, WHO-observations of item 7 are contradictory in themselves, because strict self-confinement and isolation were imposed already at the onset of the first wave, but inexplicably turned out entirely inefficient, resulting in a classical dynamic of epidemic flu, i.e., 4 weeks up and 7 weeks down, instead of the publicly promised “flatten the curve” with “reduced load on health service system.”
Considering items 2, 9 and 11, SARS-CoV-2 is physically akin to other flu viruses, and its RNA mutates at a similar rate due to RNA reproduction errors in human cells. Therefore, it is unable to produce significantly different variants capable of overcoming the existing immunity much faster than common cold and
other seasonal respiratory viruses, where such major variants come up once in a few years at least. Indeed, dozens of variants of influenza A exist, with immunologically different updates to those major variants taking many years to appear, which
explains large intervals between severe outbreaks of influenza A. Therefore, the explanation provided by WHO- consensus hypothesis must be erroneous.
Moreover, considering items 6 and 10, any public health measures cannot affect SARS-CoV-2 any differently from common cold and other seasonal respiratory viruses, for the simple reason that all these viruses are physically indistinguishable and can only propagate within aqueous droplets, losing virility once the droplets dry out. Therefore, if a surgical mask can stop one of the viruses because it stops all droplets, it will similarly stop all others. In fact, we have known for more than 100 years that masks do not affect influenza propagation. Therefore, the explanation provided by the WHO is quite demonstrably untrue.
From experimental evidence item 11, infection statistics for UK and Israel, is inconsistent at the time of writing. Figure 1 shows that the plot of new COVID-19 cases in Israel and UK, which were the most vaccinated countries, almost all adult population, at the time of writing.

Note that Israel has slightly higher percentage of complete vaccination than UK, yet lower PCR-positive case numbers at present. However, in Israel, the apparent case infection rate is growing faster than in UK and is set to overcome UK numbers in the matter of weeks. Therefore, vaccination has no apparent effect on the development of the current case numbers, exactly as predicted by the false-positive explanation.
Finally, we also note that WHO-consensus and OPS-explanation produce very different predictions of the future development of the Covid-19 pandemics, and very
different public health recommendations. We discuss these differences in the last section on conclusions and recommendations.
EXCESS MORTALITIES
Note that there are no valid RNA tests capable of discriminating covid-19 from other flu-like diseases, as demonstrated above. Therefore, no information on epidemiology of covid-19 may be obtained from published case statistics, which is all based on RNA tests. For these reasons, excess mortality statistics was considered instead. Excess mortality usually exhibits peaks associated with viral respiratory diseases in autumn
and winter seasons. However, additional peaks appeared in spring in the years 2020 and 2021, attributable to SARS-COV-2 as will be discussed below.
Eastern Europe
Figure 2 shows excess mortality in selected Eastern European countries in 2020. Apparently, these countries did not have adequate meteorological conditions for covid-19 transmission in spring of 2020, and therefore had no significant associated mortality in that period. This demonstrates that even in its first outbreak, SARS-COV-2 was transmitted as a seasonal flu virus, requiring adequate meteorological conditions, and was not transmitted outside its preferred season, contrary to what may be inferred from statistics of the new cases derived from invalid RNA tests. It is therefore concluded that SARS-COV-2 is only prevalent in spring, in the same way as all of the previously known human coronaviruses.
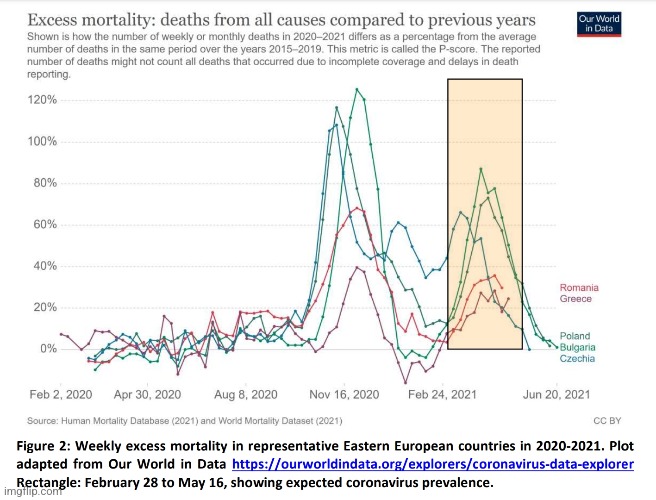
Thus, within the time interval considered, Eastern European countries had a rhinovirus peak in autumn of 2020 and their first coronavirus peak in spring 2021.
Czechia also had a discernible flu A peak, with its maximum on January 10. It is possible that rhinovirus mortality was amplified by clinical diagnostic errors induced by results of invalid PCR tests that signalled covid-19 in rhinovirus cases.
Western Europe
Figure 3 shows excess morality in selected Western European countries. Contrary to Eastern European countries, Western European countries apparently had suitable meteorological conditions for covid-19 outbreak already in spring of 2020 and strong peaks of excess mortality in this period. These peaks occurred during the first wave of covid-19 in Europe. The mortality peaks of the second covid-19 outbreak in spring of 2021 were significantly smaller, about 25% of the first outbreak, indicating that population-wide immunity was already quite advanced after the first outbreak. Note that other human coronaviruses do not produce strong mortality peaks in spring; therefore, their mutations should be significantly slower than those of flu A. It is therefore reasonable to expect that spring mortality peaks associated with covid-19 will also disappear in a year or two, after sufficient immunity is accumulated in the population. On the other hand, it seems reasonable that stronger coronavirus mortality peaks were associated to the newly appeared coronavirus, as has happened with SARS-COV-2. The second outbreak in UK did not appear at the same time as that in other countries, occurring probably about 2 months earlier, due to significantly different climate. The excess mortality peaks in autumn 2020 and winter 2020-2021 are attributable to rhinovirus and flu A. The small and sharp mortality peak appearing in Germany, Netherlands and France in August 2020 is attributable to the heat wave.
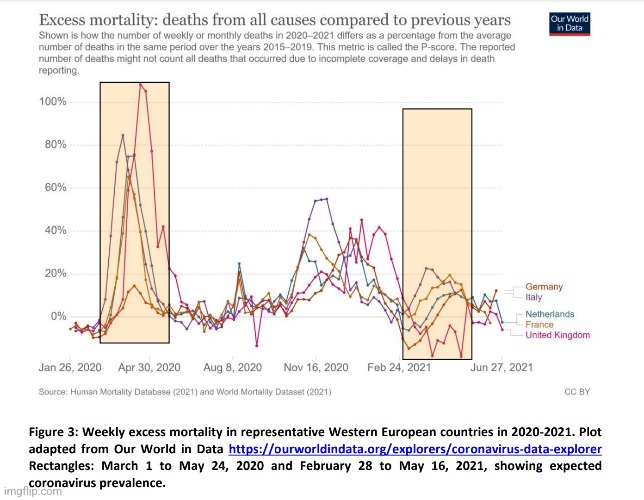
It is therefore concluded that SARS-COV-2 is quite similar to other coronaviruses, in that it appears only seasonally, in most European countries in spring, and its associated excess mortality is on the way to extinction in a few more years, indicating rapid acquisition of population-wide immunity. There are no indications of rapid mutations of this new virus, which would slow down the observed reduction in the spring excess mortality. Additional excess mortality in seasons with low SARS-COV-2 prevalence is apparently induced by utilization of the results of invalid RNA tests in the clinical practice, which leads to exaggerated scale of pandemics and misdiagnosis of other respiratory viruses as SARS-COV-2. This may cause contamination of patients already carrying a different respiratory virus by SARS-COV-2 in hospitals, where the virus may be surviving and propagating even outside its preferred season, due to the air-conditioned environment facilitating virus transfer from authentic virus carriers.
CONCLUSIONS WITH RECCOMENDATIONS
Our revised explanation for the various observations of the COVID-19 epidemiology, along with predictions for the development of Covid-19 pandemic are so far entirely consistent with all known experimental observations as evidenced by published statistical data. We have been unable, as yet, to conduct clinical experiments to confirm the reality of the MDSCV, however, researchers in St. Petersburg have obtained experimental evidence that a large fraction of COVID-19 patients has additional respiratory viruses in their system. To avoid an infinite sequence of pseudo-COVID-19 outbreaks and constant mass revaccinations, mass testing for SARS-CoV-2 and its variants should be immediately discontinued, along with futile attempts to identify asymptomatic carriers, and the respective resources used to provide remedy for chronic patients, some with other pathogens, who were
left without medical help by reorienting all medical service towards COVID-19 pandemics.
MDSCV phenomenon may be tested for in the laboratory by infecting human volunteers with known respiratory viruses other than SARS-CoV-2 and using standard
PCR tests for SARS-CoV-2 on those who develop symptoms, in a strictly quadruple-blind experimental design. In an approach not requiring volunteers, patients diagnosed with SARS-CoV-2 may be retested for seasonal respiratory viruses, which
will be present in most cases producing what is erroneously interpreted as COVID-19 due to false-positive results of PCR tests.
We are finally left with a striking contradiction between excellent specificity of SARS-CoV-2 tests demonstrated on de facto samples of other respiratory viruses in vitro as per the information provided by the test producers, and the apparently
zero specificity of the same tests revealed in vivo in clinical practice, as demonstrated here. To address this contradiction, note that all tests (and vaccines) were produced using the genetic information published by the SARS-CoV-2 discoverers in the appropriate databases.
Consulting the respective seminal publications, we find that the respective genetic material had been identified computationally without preparing an isolate of the respective virus particles, and without separating them physically from other carriers of genetic material that may be present in the biological samples. Noting that tests apparently produce false positive results in people carrying some
respiratory virus different from SARS-CoV-2, we must conclude that the alleged genetic code of the SARS-CoV-2 virus had been wrongly identified, belonging instead to something generated by human airway epithelial cells challenged with respiratory viruses and containing RNA, for instance, to exosomes, as explained above.
It is no surprise, therefore, that the tests are totally non-specific in the clinical practice, while demonstrating excellent specificity in vitro: samples of other respiratory viruses used for in vitro trials were not contaminated with products of human cells, whereas all biological samples used to identify RNA code of SARS-CoV-2 have been in contact with such cells. Note also that SARS-CoV-2 RNA had been identified by its similarity to that of another virus, which casts reasonable doubts on that previous identification.
It appears also that the RNA codes of SARS-CoV-2 variants, very similar to that of the original COVID-19 virus, have also been wrongly identified. Given that the alleged SARS-CoV-2 RNA is in fact generated by human airway epithelial cells used for virus culturing, it is possible to explain high rates of false negative results in Covid-19 patients. RNA induced by the virus in challenged human cells may vary from patient to patient, due to individual genetic differences, making it not recognizable by the test.
Having established an erroneous identification of the genetic material belonging to SARS-CoV-2, we can interpret low success rates of all the existing vaccines, requiring multiple doses to produce reasonable immune response. Indeed, the vaccines are based on the genetic material, probably exosomes, generated in human airway epithelial cells challenged by respiratory viruses, and not on the genetic material of the SARS-CoV-2 virus itself. Immunity generated by such vaccines can only act in advanced stages of Covid-19 illness, amplifying the already existing
response of the patient immune system, which could be too late for patients whose immune reaction is belated. These vaccines may also exacerbate problems in patients with other diseases that induce cell response akin to that generated by respiratory viruses, probably explaining some of the adverse reactions to vaccination amongst younger recipients.

In Summary:
- National governments’ prevention response decisions are based upon detection statistics from PCR tests that are used to define numbers of “Covid-19:”
- Infected persons
- Hospitalisations
- Deaths
- These statistics assume a priori that PCR tests are nigh 100% true detectors of “COVID-19” infections
- The researchers extracted from the published literature on PCR-test outcomes graphical data that reveals the evidence for a very large percentage of false positive results
- They hypothesized that exosomes, triggered by all “viral” respiratory infections, are largely responsible for positive outcomes from PCR-tests for “COVID-19”
- In other words, they are using one fictional entity (exosomes) to explain away another fictional entity (“viruses”)
- They found that PCR testing data for the second and following waves of “COVID-19” pandemic indicated that these waves are mainly artefacts of false-positive results
- The RNA code counted in PCR tests, previously attributed to “SARS-CoV-2,” belongs instead to a “respiratory-virus-induced immune system response” by human cells that liberate exosomes, and that vitiate PCR test results
- Recently the World Health Organisation (WHO) published a document that called attention to the relevance of false positive results of Reverse transcription (RT-) Polymerase Chain Reaction, (PCR) tests for a “SARS-CoV-2 virus”
- The WHO publication is a reminder that the disease prevalence alters the predictive value of test results
- As disease prevalence decreases, the risk of false positive increases
- In layman terms, technical specifications provided by test producers becomes irrelevant at low “SARS-CoV-2” prevalence
- The producers may claim their test is 100% specific to the “SARS-CoV-2 virus,” but in practice if “COVID-19” prevalence in the population is low or zero, each and every positive result will be a false positive, reducing the amount of information contained in it to zero
- In reality, as “Covid-19” cannot be diagnosed clinically due to overlapping symptoms with other diseases and must be confirmed molecularly, disease prevalence will never be known and all positives are false-positives as I detailed here.
- Note, however, that since the start of the pandemic, the WHO has been proclaiming that more extensive testing is necessary, which could conceivably generate ever repeating unreal ‘COVID-19 outbreaks’
- The researchers established 4 Facts at the outset:
- Irrespective of the test specificity claimed by the test manufacturer, PCR tests produce false positive results in appreciable numbers
- The fraction of false positive results in all positive results increases as the prevalence of the “SARS-CoV-2 virus” in the population decreases, e.g. due to seasonality of all other respiratory infections
- In the limiting case of zero prevalence of “SARS-CoV-2 virus,” all positive PCR test results will inevitably be false positives
- PCR tests can never indicate that “SARS-CoV-2 virus” went out of circulation, as false positives will be appearing indefinitely, indicating alleged presence of the “virus”
- The researchers found that the prevailing interpretation of PCR test results does not withstand scientific scrutiny in the light of the experimental or factual observations
- The important role of exosomes in the functioning of the immune system challenged by a “viral” respiratory disease is established science, although the precise function and molecular mechanisms remain a topical research question (so….not established science then…)
- The immune response to respiratory “viruses” is evidently triggered by the appearance of exosomes
- The trigger may also involve individual airway epithelial cells
- The exosome RNA structure is probably independent of the pathogenic “virus” and varies only in conformity with the patients’ individual genome
- These patient genome variations consistently explain several observations, which the consensus hypothesis attributes to the special properties of “SARS-COV-2”
- Any test would produce negative outcome for exosomes whose RNA is different from that of the exosomes used for developing the test
- On the other hand, sequencing of the perceived “viral” RNA in remote locations necessarily reveals new exosome strains, caused by human genetic variability, but misidentified as new “SARS-COV-2” variants
- Once tests detecting such exosomes are developed and deployed, these perceived “virus” variants get instantly discovered everywhere, creating a false and terrifying impression of their fast propagation
- These variant-specific tests would also produce false negatives on patients with differing genomes, albeit on genomes different from the undetectable genomes of the original tests
- The exosome origin of the RNA attributed to “SARS-COV-2” and its variants explains the fact that PCR tests used on patient biological samples are completely non-specific as regards the “virus”
- These tests are specific to exosome RNA, which probably carries no “virus” information, as postulated above
- This, in turn, explains a misdiagnosis phenomenon, that manifests itself in countless observations
- Illnesses caused by seasonal respiratory “viruses,” including variants of “influenza” A and B, common cold “rhinoviruses,” human “corona viruses,” etc. all being ‘misdiagnosed by PCR tests as “SARS-CoV-2 virus” (MDSCV), with very high probabilities, close to 100%
- Note that every single “virus” listed above also uses PCR for detection and all face the same false-positive problem based upon unknown disease prevalence, thus they are all false-positives as well
- The scientific method has not been adhered by scientific advisors to many national governments that have already answered “yes” to the many questions raised by the WHO in ad hoc knee-jerk responses to the pandemic
- Unlike WHO, the researchers state that they are not using any alleged or unsubstantiated properties, e.g., hypothetical rate-of-transmission of “SARS-CoV-2 variants”
- They refer only to information demonstrably correct and question the reliability of analytical tools existing at the present time, like dubious PCR tests
- However, the proposed role of exosomes in the false-positive PCR test results will remain a hypothesis that needs to be investigated with some circumspection for more direct laboratory experimental evidence that it is the agent responsible for vitiating PCR test results
- The WHO interpretations require the following hypothetical assumptions for which there is presently no compelling evidence: going against the principle of Occam’s razor:
- Transmission by asymptomatic “COVID-19” carriers
- Tests working and being 100% specific in clinical in vivo practice
- Vaccines are effective: vaccinated people are getting ‘infected’.
- Effectiveness of vaccines defined by PCR test?
- The same “virus” generating completely different outbreak dynamics in the first and subsequent waves. The OPS explanations only assume established scientific knowledge that has been conclusively demonstrated:
- PCR Tests produce false positives both on different respiratory “viruses” and on patients having no respiratory “viruses” at all
- Contact PCR testing amplifies number of tests and of false positives
- Classic, or nearly Gaussian, dynamics of the first (“SARS-CoV-2”) wave in 2020 (March-May in Western Europe), and the slower-skewed testing–generated dynamics in the subsequent waves
- The observations and consensus interpretations are somewhat contradictory
- Explanations provided by WHO- consensus hypothesis must be erroneous
- Any public health measures cannot affect “SARS-CoV-2” any differently from common cold and other seasonal respiratory “viruses,” for the simple reason that all these “viruses” are physically indistinguishable and can only propagate within aqueous droplets, losing virility once the droplets dry out
- If a surgical mask can stop one of the “viruses” because it stops all droplets, it will similarly stop all others
- However, it has been known for more than 100 years that masks do not affect influenza propagation and thus the explanation provided by the WHO is quite demonstrably untrue
- When comparing UK and Israel data, vaccination has no apparent effect on the development of the current case numbers, exactly as predicted by the false-positive explanation
- There are no valid RNA tests capable of discriminating “Covid-19” from other flu-like diseases
- Eastern European countries apparently did not have adequate meteorological conditions for “Covid-19” transmission in spring of 2020, and therefore had no significant associated mortality in that period
- This demonstrates that even in its first outbreak, “SARS-COV-2” was transmitted as a seasonal flu “virus,” requiring adequate meteorological conditions, and was not transmitted outside its preferred season, contrary to what may be inferred from statistics of the new cases derived from invalid RNA tests
- It is possible that in Eastern European countries, “rhinovirus” mortality was amplified by clinical diagnostic errors induced by results of invalid PCR tests that signalled “Covid-19” in “rhinovirus” cases
- Contrary to Eastern European countries, Western European countries apparently had suitable
- meteorological conditions for “Covid-19” outbreak already in spring of 2020 and strong peaks of excess mortality in this period
- This seasonality of disease peaking in colder months is a long-known phenomenon and does not require any “virus” to explain
- The researchers note that other human “coronaviruses” do not produce strong mortality peaks in spring; therefore, their mutations should be significantly slower than those of flu A
- It is therefore concluded that “SARS-COV-2” is quite similar to other “coronaviruses” in that it appears only seasonally
- Additional excess mortality in seasons with low “SARS-COV-2” prevalence is apparently induced by utilization of the results of invalid RNA tests in the clinical practice, which leads to exaggerated scale of pandemics and misdiagnosis of other respiratory “viruses” as “SARS-COV-2”
- Researchers in St. Petersburg have obtained experimental evidence that a large fraction of “COVID-19” patients has additional respiratory “viruses” in their system
- To avoid an infinite sequence of “pseudo-COVID-19 outbreaks” and constant mass revaccinations, mass testing for “SARS-CoV-2” and its variants should be immediately discontinued
- Futile attempts to identify asymptomatic carriers and the respective resources used to provide remedy for chronic patients, some with other pathogens, who were left without medical help by reorienting all medical service towards “COVID-19” pandemics should also be discontinued
- Patients diagnosed with “SARS-CoV-2” may be retested for seasonal respiratory “viruses,” which will be present in most cases producing what is erroneously interpreted as “COVID-19” due to false-positive results of PCR tests
- There is a striking contradiction between excellent specificity of “SARS-CoV-2” tests demonstrated on de facto samples of other respiratory “viruses” in vitro (in the lab; outside a living organism) as per the information provided by the test producers, and the apparently zero specificity of the same tests revealed in vivo (in a living organism) clinical practice
- Consulting the respective seminal publications, the researchers found that the respective genetic material had been identified computationally without preparing an isolate of the respective “virus” particles, and without separating them physically from other carriers of genetic material that may be present in the biological samples
- Noting that tests apparently produce false positive results in people carrying some respiratory “virus” different from “SARS-CoV-2,” they concluded that the alleged genetic code of the “SARS-CoV-2 virus” had been wrongly identified, belonging instead to something generated by human airway epithelial cells challenged with respiratory “viruses” and containing RNA, for instance, to exosomes
- In other words, the “SARS-COV-2 ” genome is a computer-generated stitched together Frankenstein creation from multiple sources of RNA…as many of us have been saying from the start
- It is no surprise that the tests are totally non-specific in the clinical practice
- Note also that “SARS-CoV-2” RNA had been identified by its similarity to that of another “virus,” (“SARS-COV-1”) which casts reasonable doubts on that previous identification
- It appears also that the RNA codes of “SARS-CoV-2” variants, very similar to that of the original “COVID-19 virus,” have also been wrongly identified
- The alleged “SARS-CoV-2” RNA is in fact generated by human airway epithelial cells used for “virus” culturing
- Having established an erroneous identification of the genetic material belonging to “SARS-CoV-2,” they interpreted low success rates of all the existing vaccines, requiring multiple doses to produce reasonable immune response
- These vaccines may also exacerbate problems in patients with other diseases that induce cell response akin to that generated by respiratory “viruses,” probably explaining some of the adverse reactions to vaccination amongst younger recipients

Sharing information similar to the above study will get one labelled as an uncaring and crazy conspiracy theorist. Instead of people looking critically and logically at the evidence provided, ones character will be attacked in order to shoot the messenger so that they can avoid having to understand and comprehend the message. The term conspiracy theorist was derived to drown out the voices of the opposition so that those who are in control can maintain their carefully crafted narrative. Opposing viewpoints with legitimate information and concerns are immediately disregarded as misinformation. Even sharing data and quotes directly from the institutions said to be trustworthy, such as the CDC, the FDA, and the WHO, can get one censored if it is damaging to the mainstream propaganda. For a recent example, posting the laundry list of side-effects from Pfizers own vaccine study is a guaranteed ban on Facebook as the information is considered misinformation and damaging to the community. It is time to realize that the only community being damaged and protected by the social media mafia is the pharmaceutical companies. It is time to throw away the derogatory label “conspiracy theorist” and let the information presented speak for itself.

The “isolation” of the “virus”and the evidence of the genome sequence are the fundamental criteria used by the pharmaceutically-controlled propagandists to claim that “SARS-COV-2” actually exists. As the above researchers admit that “SARS-COV-2” was never properly purified and isolated and that the genome sequence is a fraudulent model created from a mixture of RNA from various unknown sources, there can be no “SARS-COV-2” as it fails to meet the two essential requirements provided as evidence for its existence. As the PCR tests, which were used to create the increasing cases which were in turn used to claim a worldwide pandemic, were built and calibrated to a fictional “viral” genome, the only logical conclusion one can make is that all results generated are false and that we have a Testing Pandemic and not a “viral” one. Thus there is and never was any benefit to lockdowns, quarantines, social distancing, masking, vaccination, passports/tracking, etc. The information we are presenting should no longer be viewed as a conspiracy theory. It is simply facts that counter the accepted and approved mainstream fiction.

Hi, at the link below the paper is classified as PREPRINT, and as Manuscript Draft, and, of course as you can read, preprints and early-stage research may not have been peer reviewed yet. ; https://www.researchgate.net/publication/355972541_The_Lancet_Respiratory_Medicine_Role_of_exosomes_in_false-positive_covid-19_PCR_tests
The website you linked, Academia, is just “the easiest way to share papers with millions of people across the world for free.” as they say.
I tried to find it in Pubmed and The Lancet Respiratory Medicine, but I couldn’t find it.
The study seems interesting but how can we be sure that this paper has been published in The Lancet Respiratory Medicine with proper peer review?
LikeLike
Yes, it is a preprint. It says it was submitted to The Lancet as it has a manuscript number:
thelancetrm-D-21-01205
https://www.researchgate.net/publication/355972541_The_Lancet_Respiratory_Medicine_Role_of_exosomes_in_false-positive_covid-19_PCR_tests
It will definitely be interesting to see if it will survive the peer review process in order to be fully published. I doubt it will. However, peer review or not, the information contained within is well referenced and provides evidence against the MSM narrative. It was submitted in November 2021. Most studies of this type never seem to last that long without some form of disclaimer attempting to discredit the information within.😉
LikeLiked by 1 person
Totally agree. Is it interesting to compare the peer review process of this paper with the peer review process of the fraudulent paper on Covid 19 PCR test by Corman and Drosten published in Eurosurveillance , where this guys said: “We aimed to develop and deploy robust diagnostic methodology for use in public health laboratory settings without having virus material available.”
In fact, afterwards it has been discovered that: “Finally, the very short timescale between submission and acceptance of the publication (24 hours) signifies that a systematic peer review process was either not performed here, or of problematic poor quality. ”
https://cormandrostenreview.com/report/
LikeLiked by 3 people
Great point! They can rush the Drosten PCR paper through peer review in less than 24 hours but this paper is seemingly stuck in limbo. There couldn’t be any hidden agenda now could there? 😉
LikeLiked by 2 people
I note all three authors are critical of the climate change narrative. That probably makes them non-mainstream enough for a Team Science* adherent to dismiss them, unfortunately. If attention is drawn to the article there’s a substantial chance it gets taken down.
The nephrologists’ paper on how normal kidney excretions are being treated as viruses was perhaps more damning in that sense.
https://kidney360.asnjournals.org/content/1/8/824
*meaning Team Scientism
LikeLike
Pal review sunk real science awhile ago, as climate scientivism attests. Other agendas are at play as former UNFCCC Exec. Sec. Christiana Figueres stated clearly, namely, the agenda to intentionally transform the current economic and industrial model of the West through an environmental (climatism) agenda.
The recent Pfizer study published in the NEJM alleging clot-shot efficacy in children is a case in point. Of the first four authors, two are not listed as investigators in the appendix, while one of those two is touted as the corresponding author. Both unsurprisingly are Pfizer employees.
Spinmeisters anyone?
LikeLiked by 1 person
It’s a corrupt and incestuous system where the pharmaceutical companies prop up their own findings and results with their own people published in their own journals while drowning out any dissent.
LikeLike
“… mass testing for SARS-CoV-2 and its variants should be immediately discontinued” Someone better tell Uncle Joe to abandon the “test and treat” initiative he announced during the State of Confusion speech. From the Washington Post, test and treat will, “… allow patients to get tested for the coronavirus at pharmacies and, if positive, receive oral antiviral pills immediately at no cost.” How fantastic! Go to the drug store (feeling ill or not), take a bogus test for a non-existent virus and if you test positive, go home with “free” toxic, rushed-to-market emergency-use authorized oral antiviral pills to take. To keep you from getting sick(er) from the non-existent virus. Yay!
LikeLiked by 2 people
Wow, I missed all of that. I pretty much ignore Biden these days. What a shit show this has become.
LikeLike
I didn’t watch/listen live, but had great fun hearing him being harpooned on several podcasts the next day. Also saw a few video clips, very painful.
From the Daily Mail, 2 March 2022, “President Joe Biden said Tuesday night that Americans’ access to highly effective antiviral Covid pills will be increased under a new ‘Test to Treat’ plan being rolled out by the federal government, and that the pills that were once in short supply should soon be readily available in the U.S., as officials make a strong push to put the pandemic in the rear view.
Speaking to congress at the State of the Union address, the President announced that the country had increased its purchase order of Pfizer’s Paxlovid from 10 million to 20 million courses. The drug, which received authorization from the Food and Drug Administration (FDA) late last year, has been deemed as the most effective treatment post-infection but the company has reportedly had issues with production.
‘If you get COVID-19, the Pfizer pill reduces your chances of ending up in the hospital by 90 percent,’ Biden said.”
There you have it. A miracle pill as a chaser to the magic jab.
LikeLiked by 1 person
“Authorized,” meaning there will be more variants to justify its use otherwise the pills will be illegal.
LikeLike
Holy mackerel, it’s the new AIDS. If that catches on, oh boy… we’re in for a lot more disease, probably blamed on a new “virus” (or maybe just HIV again).
LikeLiked by 1 person
“Trust only official, verified sources!” (Trust only the sources that already agree with me!)
Anyway, I’ve heard that “the seal of God is truth,” so, “the seal of the government and mainstream propaganda is bullshit, so disconnected from reality that they are even beyond lies.” (Doesn’t quite roll off the tongue)
LikeLiked by 1 person
It might not roll off the tongue but it is very accurate nonetheless! 😉
LikeLike
Nothing to argue here. But what you describe is pretty much an outline that permeates the entire medical complex. Create the disease, illness or malady, then create fear ( the fear of death) and they will come with open hearts, minds and wallets insisting that they be cured, or at least spared a gruesome, horrendous death.
The believers have been brainwashed for decades and would never question the almighty practitioners of medicine, often heralded as miracle workers, though that is mostly fantasy and propaganda.
I have been reading the book “Mad In America” and it is the same in the mental health fields. I really have to wonder who was more insane?…the patients or the doctors and their horrific treatments.
LikeLiked by 1 person
My money is on the doctors, or at the very least anyone identifying as virologists. 😉
LikeLike
Thanks Mike.
May also want to check out the Dsalut article, may have already seen it,
Click to access The-scam-has-been-confirmed-Dsalud-November-2020.pdf
Was looking up something and looked up again this article from Nov 2020.
Before the covid scam I have not really looked into the PCR and new nothing about it. . It does not take long to figure out what is going on.
Most likely physicians do not care to question and scientists are on the gravy train.
“Financial incentives can compromise the critical faculties of an individual. Here are four versions of this insight:
Never argue with a man whose job depends on not being convinced.
It is difficult to get a man to understand something, when his salary depends upon his not understanding it.
It can be very hard to understand something, when misunderstanding it is essential to your paycheck.
It is rather pointless to argue with a man whose paycheck depends upon not knowing the right answer.”
Source: https://quoteinvestigator.com/2017/11/30/salary/
LikeLiked by 1 person
Was just listening to this video
—-
Here are some figures to put into context.
Last updated: July 29, 2022, 21:59 GMT
China
Coronavirus Cases:
229,294
Deaths:
5,226
Recovered:
222,314
https://www.worldometers.info/coronavirus/country/china/
——
Last updated: July 29, 2022, 21:59 GMT
United Kingdom
Coronavirus Cases:
23,304,479
Deaths:
183,953
Recovered:
22,613,397
——
Figure that out. they are not testing or using low cycles as they must know the test is a farce.
The Chinese has a booming economy so will set an example as a great country to follow its social credit system .🤔
https://www.worldometers.info/coronavirus/country/uk/
LikeLike
Positive PCR
https://t.me/NEXTLEVEL_OnlineForum/8957/28399
There are several reasons why someone tests positive. Some of them are:
What is detected in the PCR are not complete “genomes”, but only very short sequence sections, usually between 200 – 300 nucleotides. But often only very short < 40 nt. This does not prove anything specific, but a believed specific area that is scientifically untenable. Many institutions and a member of the Drosten team have now confirmed this.
Factors for positive results
1. The number of cycles (cut-off setting) can affect the measurement. The more cycles are run, the more useless the results become.
2. Contamination of the test kits that are used. There have already been several cases in the media showing that a whole group tested positive because of contaminated test kits.
3. There are many hundreds of different PCR tests, from different companies. From a purely technical point of view, most of them are of very poor quality in terms of their specificity.
4. There is no calibration of the tests, neither on the so-called cut-off value (number of cycles), nor on the primers and other chemicals used. This means that the person being tested may test positive in one lab, negative in another, etc
5. The PCR test kits examine a different number of "genes" that are assigned to a "virus". On the one hand, no entire "gene sections" are searched for, but only a small fraction here, and on the other hand, different tests are used to test for 1 gene (e.g. the E gene), sometimes for two or 3 genes. In the case of the E gene in particular, it is known that this does not represent a specific sequence for a corona virus and therefore has no meaningfulness without taking the other weaknesses into account.
Additional notes on why a test can be positive
Since the short pieces of nucleic acids from which the viruses are mentally assembled are released during all inflammatory processes, the build-up and breakdown and the death of tissues, it is clear that all people are tested "positive" with the PCR nucleic acid detection technique where there is inflammation, build-up, breakdown or death of tissues, and from which tissues and fluids are taken for testing.
Likewise, the test will automatically test people as positive if, when testing through the swab,
a.) too many mucous membranes are damaged,
b.) this leads to bleeding,
c.) In the nasal cavity, the very sensitive olfactory bulb, a part of the brain, is mechanically injured or
d.) simply taking a very large sample volume.
Because in the body, even in every natural body of water and in all seas, an astonishingly intensive build-up and breakdown of all kinds of nucleic acids is constantly taking place. The PCR virus test only detects very short nucleic acids that are claimed to be part of a virus.
You can find more information on our website, for example in the area of verification methods. More articles will be published there in the near future. Some are reserved for our subscribers.
LG
NEXT LEVEL – Knowledge rethought
http://www.wissen-neu-thought.de
LikeLike